The Project Gutenberg EBook of The Mother and Her Child, by
William S. Sadler and Lena K. Sadler
This eBook is for the use of anyone anywhere at no cost and with
almost no restrictions whatsoever. You may copy it, give it away or
re-use it under the terms of the Project Gutenberg License included
with this eBook or online at www.gutenberg.org
Title: The Mother and Her Child
Author: William S. Sadler
Lena K. Sadler
Release Date: March 14, 2007 [EBook #20817]
Language: English
Character set encoding: ISO-8859-1
*** START OF THIS PROJECT GUTENBERG EBOOK THE MOTHER AND HER CHILD ***
Produced by Audrey Longhurst, Hillie Plantinga and the
Online Distributed Proofreading Team at http://www.pgdp.net
Seven typographical errors have been corrected, this is indicated in the html like this, hover with the mouse over the word for an explanation.
THE MOTHER
AND HER CHILD
BY
WILLIAM S. SADLER, M. D.
PROFESSOR OF THERAPEUTICS, THE POST-GRADUATE MEDICAL
SCHOOL OF CHICAGO; DIRECTOR OF THE CHICAGO INSTITUTE
OF PHYSIOLOGIC THERAPEUTICS; FELLOW OF THE
AMERICAN MEDICAL ASSOCIATION; MEMBER OF
THE CHICAGO MEDICAL SOCIETY; THE ILLINOIS
STATE MEDICAL SOCIETY; THE AMERICAN
ASSOCIATION FOR THE ADVANCEMENT
OF SCIENCE, ETC.
AND
LENA K. SADLER, M. D.
ASSOCIATE DIRECTOR OF THE CHICAGO INSTITUTE OF PHYSIOLOGIC
THERAPEUTICS; FELLOW OF THE AMERICAN MEDICAL
ASSOCIATION; MEMBER OF THE CHICAGO MEDICAL
SOCIETY; THE MEDICAL WOMEN'S CLUB OF CHICAGO;
NATIONAL CONGRESS OF MOTHERS AND
PARENT-TEACHER ASSOCIATION; THE
CHICAGO WOMAN'S CLUB, ETC.
ILLUSTRATED

TORONTO
McCLELLAND, GOODCHILD & STEWART
CHICAGO: A. C. McCLURG & CO.
1916
Copyright
A. C. McClurg & Co.
1916
Published August, 1916
Copyrighted in Great Britain
W. F. HALL PRINTING COMPANY, CHICAGO
TO
"BILLY"
WHO, BECAUSE OF HIS UNCONSCIOUS CONTRIBUTIONS TO ITS
PRACTICAL FEATURES, SHOULD BE REGARDED AS A
CO-AUTHOR, THIS VOLUME IS AFFECTIONATELY
DEDICATED BY HIS PARENTS
THE AUTHORS
For many years the call for a book on the mother and her child has come to us from patients, from the public, and now from our publishers—and this volume represents our efforts to supply this demand.
The larger part of the work was originally written by Dr. Lena K. Sadler, with certain chapters by Dr. William S. Sadler, but in the revision and re-arrangement of the manuscript so much work was done by each on the contributions of the other, that it was deemed best to bring the book out under joint authorship.
The book is divided into three principal parts: Part I, dealing with the experience of pregnancy from the beginning of expectancy to the convalescence of labor: Part II, dealing with the infant from its first day of life up to the weaning time; Part III, taking up the problems of the nursery from the weaning to the important period of adolescence.
The advice given in this work is that which we have tried out by experience—both as parents and physicians—and we pass it on to mothers, fathers, and nurses with the belief that it will be of help in their efforts at practical and scientific "child culture." We believe, also, that the expectant mother will be aided and encouraged in bearing the burdens which are common to motherhood by the advice and instruction offered.
While we have drawn from our own professional and personal experience in the preparation of this book, we have also drawn freely from the present-day literature dealing with the subjects treated, and desire to acknowledge our indebtedness to the various writers and authorities.[Pg viii]
We now jointly send forth the volume on its mission, as a contribution toward lightening the task and inspiring the efforts of those mothers, nurses, and others who honor us by a perusal of its pages.
William S. Sadler.
Lena K. Sadler.
Chicago, 1916.
PART I
THE MOTHER
| CHAPTER | PAGE | |
| I | The Expectant Mother | 1 |
| II | Story of the Unborn Child | 7 |
| III | Birthmarks and Prenatal Influence | 14 |
| IV | The Hygiene of Pregnancy | 21 |
| V | Complications of Pregnancy | 35 |
| VI | Toxemia and Its Symptoms | 47 |
| VII | Preparations for the Natal Day | 53 |
| VIII | The Day of Labor | 63 |
| index | Twilight Sleep and Painless Labor | 71 |
| X | Sunrise Slumber and Nitrous Oxid | 84 |
| XI | The Convalescing Mother | 93 |
PART II
THE BABY
| XII | Baby's Early Days | 103 |
| XIII | The Nursery | 114 |
| XIV | Why Babies Cry | 123 |
| XV | The Nursing Mother and Her Babe | 133 |
| XVI | The Bottle-Fed Baby | 147 |
| XVII | Milk Sanitation | 156 |
| XVIII | Home Modification of Milk | 165 |
| XIX | The Feeding Problem | 177 |
| XX | Baby's Bath and Toilet | 190 |
| XXI | Baby's Clothing | 202 |
| XXII | Fresh Air, Outings, and Sleep | 213 |
| XXIII | Baby Hygiene | 222 |
| XXIV | Growth and Development | 232 |
PART III
THE CHILD
| XXV | The Sick Child | 251 |
| XXVI | Baby's Sick Room | 266 |
| XXVII | Digestive Disorders | 274 |
| XXVIII | Contagious Diseases | 285 |
| XXIX | Respiratory Diseases | 300 |
| XXX | The Nervous Child | 308 |
| XXXI | Nervous Diseases | 323 |
| XXXII | Skin Troubles | 333 |
| XXXIII | Deformities and Chronic Disorders | 341 |
| XXXIV | Accidents and Emergencies | 348 |
| XXXV | Diet and Nutrition | 360 |
| XXXVI | Caretakers and Governesses | 370 |
| XXXVII | The Power of Positive Suggestions | 380 |
| XXXVIII | Play and Recreation | 390 |
| XXXIX | The Puny Child | 400 |
| XL | Teaching Truth | 405 |
| Appendix | 427 | |
| Index | 449 |
| The mother and her child | Frontispiece | |
| FIGURE | PAGE | |
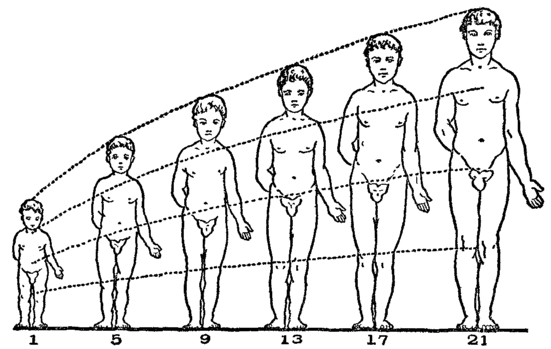
| 1 | Steps in early development | 10 |
| 2 | The "expectant" costume | 23 |
| 3 | The photophore | 43 |
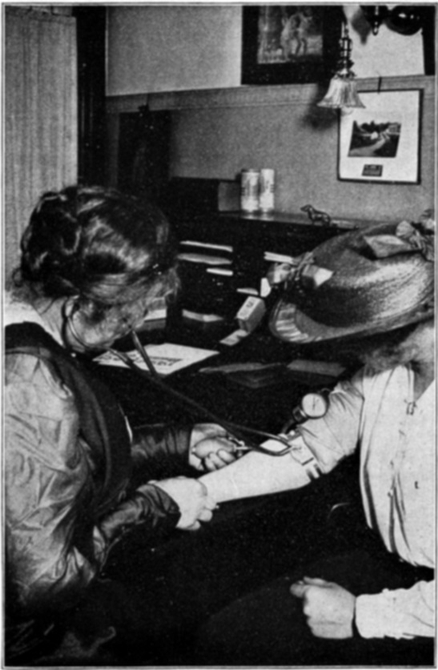
| 4 | Taking the blood pressure | 48 |
| 5 | Breast binder | 59 |
| 6 | How to hold the baby | 110 |
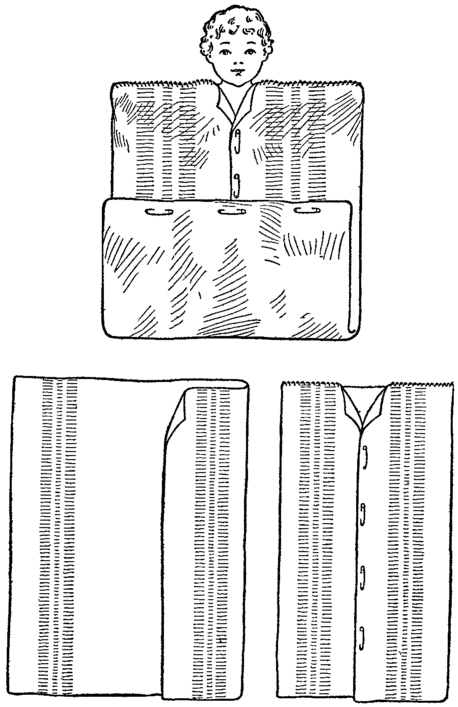
| 7 | Making the sleeping blanket | 117 |
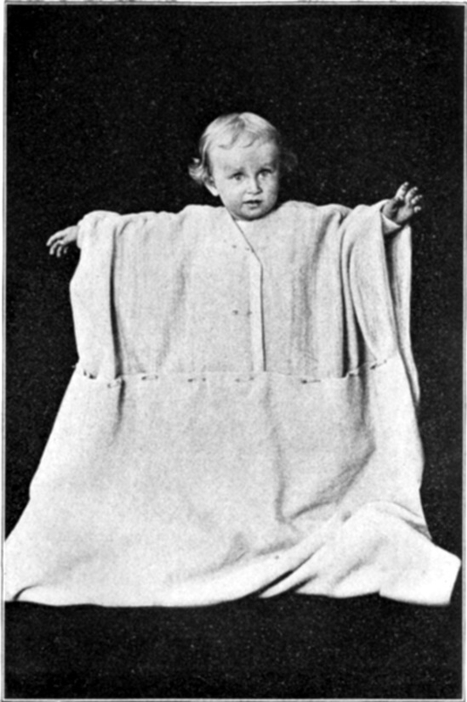
| 8 | In the sleeping blanket | 118 |
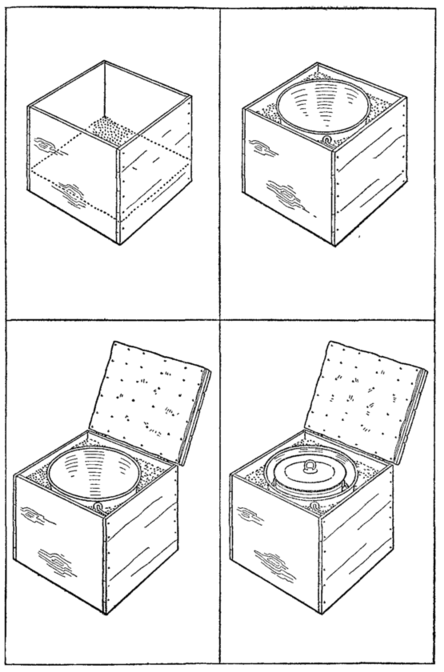
| 9 | Homemade ice box | 149 |
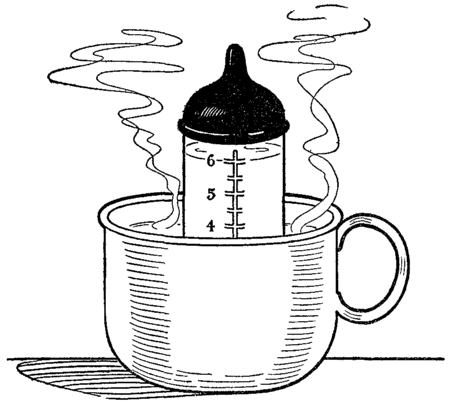
| 10 | Heating the bottle | 151 |
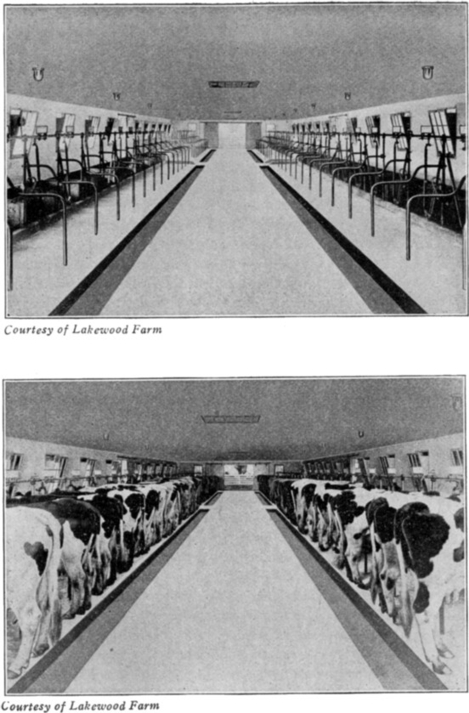
| 11 | A sanitary dairy | 158 |
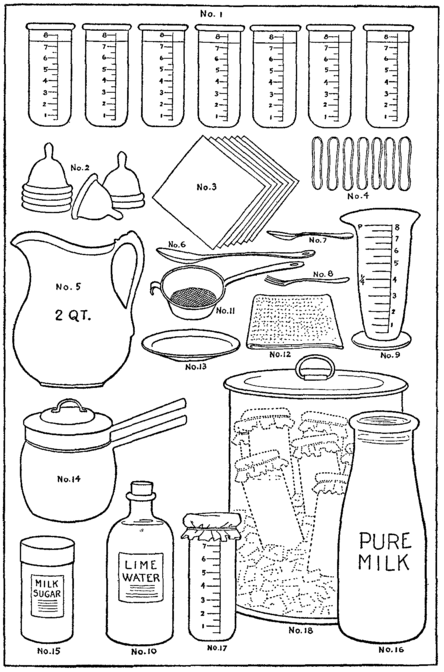
| 12 | Articles needed for baby's feeding | 167 |
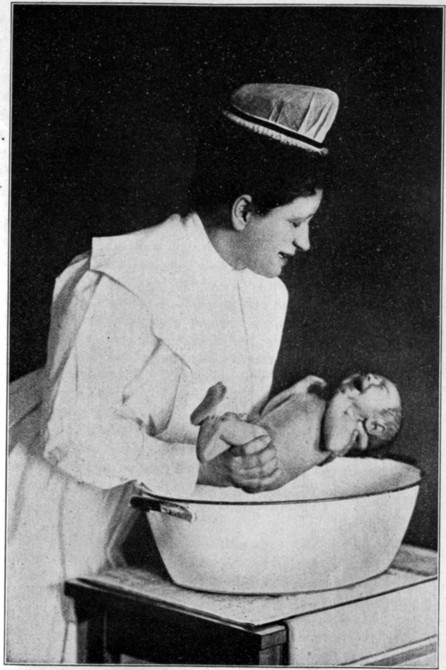
| 13 | Supporting the baby for the bath | 194 |
| 14 | Developmental changes | 240 |
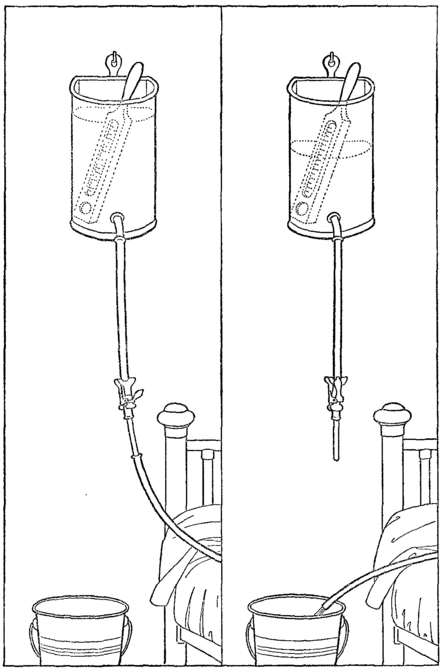
| 15 | The cooling enema | 290 |
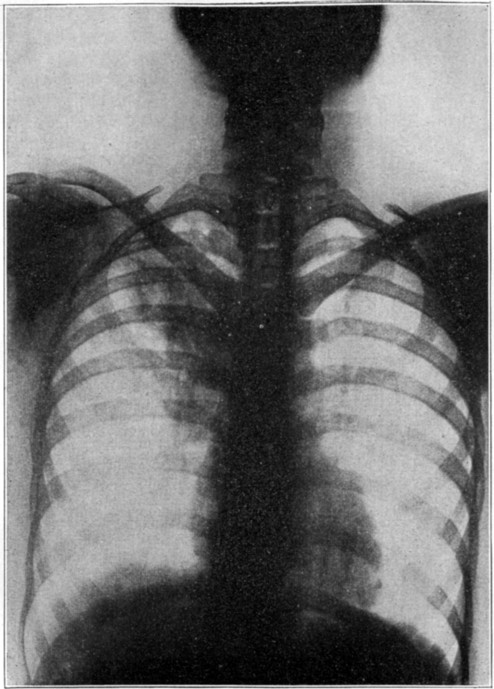
| 16 | X ray showing tuberculosis of the lung | 346 |
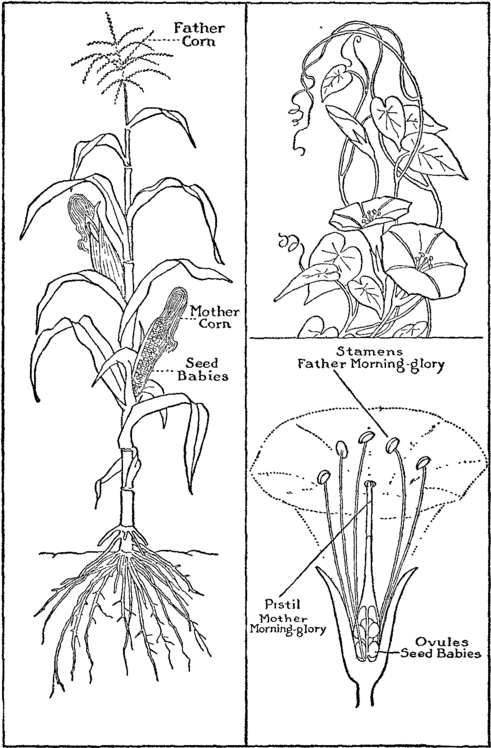
| 17 | Father and Mother Corn and Morning Glory | 406 |
There can be no grander, more noble, or higher calling for a healthy, sound-minded woman than to become the mother of children. She may be the colaborer of the business man, the overworked housewife of the tiller of the soil, the colleague of the professional man, or the wife of the leisure man of wealth; nevertheless, in every normal woman in every station of life there lurks the conscious or sub-conscious maternal instinct. Sooner or later the mother-soul yearns and cries out for the touch of baby fingers, and for that maternal joy that comes to a woman when she clasps to her breast the precious form of her own babe.
Motherhood is by far woman's highest and noblest profession. Science, art, and careers dwindle into insignificance when we attempt to compare them with motherhood. And to attain this high profession, to reach this manifest "goal of destiny," women are seeking everywhere to obtain the best information, and the highest instruction regarding "mothercraft," "babyhood," and "child culture."2
In an Indiana town not long ago, at the close of a lecture, a small, intellectual-appearing mother came forward, and, tenderly placing her tiny and emaciated infant in my arms, said: "O Doctor! can you help me feed my helpless babe? I'm sure it is going to die. Nothing seems to help it. My father is the banker in this town. I graduated from high school and he sent me to Ann Arbor, and there I toiled untiringly for four years and obtained my degree of B. A. I have gone as far as I could—spent thousands of dollars of my unselfish father's money—but I find myself totally ignorant of my own child's necessities. I cannot even provide her food. O Doctor! can't something be done for young women to preparé them for motherhood?"
The time will come when our high and normal schools will provide adequate courses for the preparation of the young woman for her highest profession, motherhood. This young mother, who had reached the goal of Bachelor of Arts, found to her sorrow that she was entirely deficient in her education and training regarding the duties and responsibilities of a mother. In every school of the higher branches of education that train young women in their late teens there should be a chair of mothercraft, providing practical lectures on baby hygiene, dress, bathing, and the general care of infants, and giving instruction in the rudiments of simple bottle-feeding, together with the caloric values of milk, gruels, and other ingredients which enter into the preparation of a baby's food.
Young women would most enthusiastically enroll for such classes, and as years passed and marriage came and children to the home, imagine the gratitude that would flood the souls of the young mothers who were fortunate enough to have attended schools where the chairs of motherhood prepared them for these new duties and responsibilities.
Just as soon as it is known that a baby is coming into the home, the expectant mother should engage the best doctor3 she can afford. She should make frequent calls at his office and intelligently carry out the instruction concerning water drinking, exercise, diet, etc. Twenty-four hour specimens of urine should be frequently saved and taken to the physician for examination. In these days the blood-pressure is closely observed, together with approaching headaches and other evidences of possible kidney complications. The early recognition of these dangers is accompanied by the immediate employment of appropriate sweating procedures and other measures designed to promote the elimination of body poisons. Thus science is able effectively to stay the progress of the high blood-pressure of former days, and which was so often followed by eclampsia—uremic poisoning.
In these days of careful urine analysis, expertly administered anaesthetics, and up-to-date hospital confinements, the average intelligent woman may enter into pregnancy quite free from the oldtime fears, whose only rewards were grief and cankering care. All fear of childbirth and all dread of maternal duties and sacrifices do not in the least lessen the necessary unpleasantness associated with normal labor. It lies in the choice of every expectant mother to journey through the months of pregnancy with dissatisfaction and resentment or with joy and serenity. "The child will be born and laid in your arms to be fed, cared for, and reared, whether you weep or smile through the months of waiting."
A little woman came into our office the day of this writing, saying: "Doctor, I'm just as mad as I can be; I don't want to be pregnant, I just hate the idea." As I smiled upon this girl-wife of nineteen, I drew from my desk a sheet of paper and slowly wrote down these words for the head of a column: "Got a mad on," and for the head of another, "Got a glad on;" and then we quickly set to work carefully to tabulate all the results that having a "mad on" would bring. We found to her dismay that its harvest would be sadness of the heart, husband unhappy, work unbearable, while all church duties as well as social functions would be sadly marred. Then, just4 as carefully, we tabulated the benefits that would follow having a "glad on." Her face broke into a smile; she laughed, and as she left the office she assured me that she would accept Nature's decree, make the best of her lot, and thus wisely align herself with the normal life demands of old Mother Nature. This view of her experience, she came to see, would bring the greatest amount of happiness to both herself and husband. She left me, declaring that she was just "wild for a baby;" and there is still echoing in my ears her parting words: "I'm leaving you, Oh, such a happy girl! and I'm going home to Harold a happy and contented expectant mother."
There often enters on the exit of a discontented and resentful expectant mother, a woman, very much alone in the world—perhaps a bachelor maid or a barren wife, who, as she sits in the office, bitterly weeps and wails over her state of loneliness or sterility; and so we are led to realize that discontentment is the lot of many women; and we are sometimes led to regret that ours is not the power to take from her that hath and give to her that hath not.
Among the first questions an expectant mother asks is: "What are early signs of pregnancy?" The answer briefly is:
Menstruation may be interrupted by other causes than pregnancy, but the missing of the second or third periods usually indicates pregnancy. Accompanying the cessation of menstruation, changes in the breast occur. Sensation in the breasts akin to those which usually accompany menstruation are manifested at this time in connection with the unusual sensations of stinging, prickling, etc. Fully one-half of our patients do not suffer with "morning sickness;" however, it is the general consensus of opinion that "morning sickness" is one of the5 early signs of pregnancy, and these attacks consist of all gradations—from slight dizziness to the most severe vomiting. It is an unpleasant experience, but in passing through it we may be glad in the thought that "it too, will pass."
Because of the pressure exerted by the growing uterus upon the bladder, disturbances in urination often appear, but as the uterus continues to grow and lifts itself up and away from the bladder these symptoms disappear.
Chief of the later signs of pregnancy are "quickening" or fetal movements. The movements are very much like the "fluttering of a young birdling." They usually are felt by the expectant mother between the seventeenth and eighteenth weeks. This sign, together with the noting of the fetal heartbeat at the seventh month, constitute the positive signs of pregnancy.
And now our expectant mother desires to know when to expect the little stranger. From countless observations of childbirth under all conditions and in many countries, the pregnant period is found to cover about thirty-nine weeks, or two hundred and seventy-three days. There are a number of ways or methods of computing this time. Many physicians count back three months and add seven days to the first day of the last menstruation. For instance, if the last menstruation were December 2 to 6, then, to find the probable day of delivery, we count back three months to September 2, and then add seven days. This gives us September 9, as the probable date of delivery. The real date of delivery may come any time within the week of which this calculated date is the center.
As a rule, ten days to two weeks preceding the day of delivery, the uterus "settles" down into the pelvis, the waist line becomes more comfortable, and the breathing is much easier.
On the accompanying page, may be found a table for computing the probable day of labor, prepared in accordance with the plan just described.6
TABLE FOR CALCULATING THE DATE OF CONFINEMENT
| Jan. | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | 24 | 25 | 26 | 27 | 28 | 29 | 30 | 31 | |
| Oct. | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | 24 | 25 | 26 | 27 | 28 | 29 | 30 | 31 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | Nov. |
| Feb. | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | 24 | 25 | 26 | 27 | 28 | ||||
| Nov. | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | 24 | 25 | 26 | 27 | 28 | 29 | 30 | 1 | 2 | 3 | 4 | 5 | Dec. | |||
| Mar. | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | 24 | 25 | 26 | 27 | 28 | 29 | 30 | 31 | |
| Dec. | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | 24 | 25 | 26 | 27 | 28 | 29 | 30 | 31 | 1 | 2 | 3 | 4 | 5 | Jan. |
| April. | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | 24 | 25 | 26 | 27 | 28 | 29 | 30 | ||
| Jan. | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | 24 | 25 | 26 | 27 | 28 | 29 | 30 | 31 | 1 | 2 | 3 | 4 | Feb. | |
| May. | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | 24 | 25 | 26 | 27 | 28 | 29 | 30 | 31 | |
| Feb. | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | 24 | 25 | 26 | 27 | 28 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | Mar. |
| June. | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | 24 | 25 | 26 | 27 | 28 | 29 | 30 | ||
| Mar. | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | 24 | 25 | 26 | 27 | 28 | 29 | 30 | 31 | 1 | 2 | 3 | 4 | 5 | 6 | April. | |
| July. | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | 24 | 25 | 26 | 27 | 28 | 29 | 30 | 31 | |
| April. | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | 24 | 25 | 26 | 27 | 28 | 29 | 30 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | May. |
| Aug. | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | 24 | 25 | 26 | 27 | 28 | 29 | 30 | 31 | |
| May. | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | 24 | 25 | 26 | 27 | 28 | 29 | 30 | 31 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | June. |
| Sept. | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | 24 | 25 | 26 | 27 | 28 | 29 | 30 | ||
| June. | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | 24 | 25 | 26 | 27 | 28 | 29 | 30 | 31 | 1 | 2 | 3 | 4 | 5 | 6 | July. | |
| Oct. | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | 24 | 25 | 26 | 27 | 28 | 29 | 30 | 31 | |
| July. | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | 24 | 25 | 26 | 27 | 28 | 29 | 30 | 31 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | Aug. |
| Nov. | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | 24 | 25 | 26 | 27 | 28 | 29 | 30 | ||
| Aug. | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | 24 | 25 | 26 | 27 | 28 | 29 | 30 | 31 | 1 | 2 | 3 | 4 | 5 | 6 | Sept. | |
| Dec. | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | 24 | 25 | 26 | 27 | 28 | 29 | 30 | 31 | |
| Sept. | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | 24 | 25 | 26 | 27 | 28 | 29 | 30 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | Oct. |
Supposing the upper figure in each pair of horizontal lines to represent the first day of the last menstrual period, the figure beneath it, with the month designated in the margin, will show the probable date of confinement.
To every physician in every community, sooner or later in his experience there come thoughtless women making requests that we even hesitate to write about. Their excuses for the crime which they seek to have the physician join them in committing, range all the way from "I don't want to go to the trouble," to "Doctor, I've got seven children now, and I can't even educate and dress them properly;" or, maybe, "I nearly lost my life with the last one."
One little woman came to us the other day from the suburbs, and honestly, frankly, related this story:
"We've been married just six months, I have continued my stenographic work to add the sixty-five dollars to our monthly income. Doctor, we must meet our monthly payments on the home, I must continue to work, or we shall utterly fail. I am perfectly willing a baby shall come to us two years from now, but, doctor, I just can't allow this one to go on, you must help me just this once. Why doctor, there can't be much form or life there, it's only three months now, or will be next week, and you know it's nothing but a mass of jelly."
She had talked with a "confidential friend" in her neighborhood, had been told that she "could do it herself," but fearing trouble or infection, had come to the conclusion she had better go to a "clean, reputable physician," to have the abortion performed.
This is not the place to narrate the experiences of the unfortunate victims of habitual criminal abortion, but we would like to impress upon the reader some realization of the untimely8 deaths, the awful suffering, and the life-long remorse and sorrow of the poor, misguided women who listen to the criminal advice of neighborhood "busybodies." The infections, the invalidism, the sterility that so often follow in the wake of these practices, are well known to all medical people.
And so after the patient's last statement, "It's nothing but a mass of jelly," we began the simple but wonderfully beautiful story of the development of the "child enmothered." Just as all vegetables, fruits, nuts, flowers, and grains come from seeds sown into fertile soil, and just as these seeds receive nourishment from the soil, rain, and sunshine, so all our world of brothers and sisters, of fathers and mothers, came from tiny human seeds, and in their turn received nourishment from the peculiarly adapted stream of life, which flows in the maternal veins for the nourishment and upbuilding of the unborn embryo.
Every little girl and boy baby that comes into the world, has stored within its body, in a wonderfully organized capsule, a part of the ancestral stream of life that unceasingly has flowed down through the centuries from father to son and from mother to daughter. This "germ plasm" is a divine gift to be held in trust and carefully guarded from the odium of taint, to be handed down to the sons and daughters of the next generation. Any young man who grasps the thought that he possesses a portion of the stream of life, that he holds it in sacred trust for posterity, cannot fail to be impressed with a sense of solemn responsibility so to order his life as to be able to transmit this biologic trust to succeeding generations free from taint and disease.
Just as within the body of "Mother Morning Glory" (See Fig. 18) may be found the ovary or seed bed, so there are two wonderfully organized bodies about the size of large almonds found in the lower part of the female abdomen on either side of the uterus, and connected to it by two sensitive tubes. There ripens in one of these bodies each month a human baby-seed,9 which finds its way to the uterus through the little fallopian tube and is apparently lost in the debris of cells and mucus which, with the accompanying hemorrhage go to make up the menstrual flow. This continues from puberty to menopause, each gland alternatingly ripening its ovum, only to lose it in the periodical phenomenon of menstruation, which is seldom interrupted save by that still more wonderful phenomenon of conception.
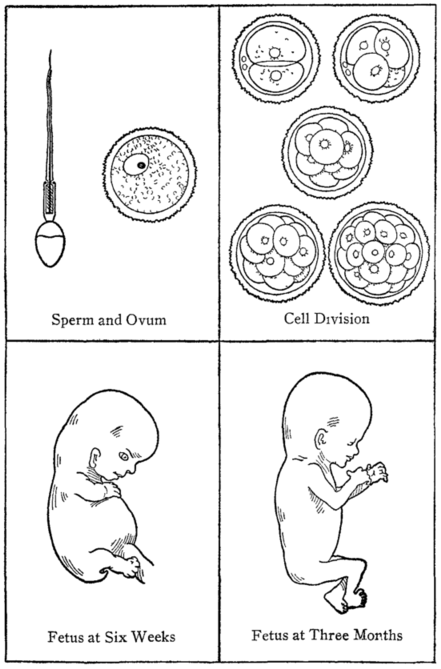
At the time of conception, countless numbers of male germ-cells (sperms) are lost—only one out of the multitude of these perfectly formed sperms made up of the mosaics of hereditary depressors, determiners, and suppressors that so subtly dictate and determine the characteristics and qualifications of the on-coming individual—I repeat, only one of these wonderful sperms finds the waiting ovum (Fig. 1). In this search for the ovum, the sperm propels itself forward by means of its tail—for the male sperm in general appearance very much resembles the little pollywog of the rain barrel (Fig. 1).
The fateful meeting of the sperm and the ovum takes place usually in the upper end of one of the fallopian tubes. It is a wonderful occasion. The wide-awake, vibrating lifelike sperm plunges head first and bodily into the ovum. The tail, which has propelled this bundle of life through the many wanderings of its long and perilous journey, now no longer needed, drops off and is lost and forgotten. This union of the male and female sex cells is called "fertilization." There immediately follows the most complete blending of the two germ cells—one from the father and one from the mother—each with its peculiar individual, family, racial, and national characteristics. Here the combined determiners determine the color of the eyes, the characteristics of the hair, the texture of the skin, its color, the size of the body, the stability of the nervous system, the size of the brain, etc., while the suppressors do a similar work in the modification of this or that family or racial characteristic.
The fertilized ovum remains in the tube for about one week, when it slowly makes its way down into the uterus, all the 11while rapidly undergoing segmentation or division. It does not grow much in size during this first week, but divides and subdivides first, into two parts, then four, then eight, then sixteen and so on, until we have a peculiar little body made up of many equally divided parts, and known as the "Mulberry Mass" (Fig. 1). The blending of the sperm and ovum has been perfect, the division of the original body multitudinous.
While this division of the united sex cells is progressing, a wonderful change is also taking place in the inside lining of the uterus. Instead of the usual thin lining, it has greatly thickened and has become highly sensitized, and as the ovum enters the uterus from the fallopian tube, this sensitized lining catches it and holds it in its folds—actually covers it with itself—holding the precious mass much as the cocoon, you have so often seen fastened to the side of a plant or leaf, holds its treasure of life.
Just as soon as the new uterine home is found the baby heart begins to make its appearance, as also do many other rudimentary parts. By the end of the third week, our round mass has flattened and curved and elongated, and the nervous system and brain begin to develop, while the primitive ears begin to appear. At this time, the alimentary canal presents itself as one straight tube which is a trifle larger at the head end. And it is interesting to note that at this early date, even the arms and legs are beginning to bud and push out from the body.
In the fourth and fifth weeks, the lungs and the pancreas may be found, the heart develops, the nervous system has taken on more definite form, and several of the larger blood-vessels are appearing.
By the eighth week, by the most wonderful and complicated processes of overlapping, pushing out, indentation, enfolding, budding, pressing, and curving, the majority of the important structures are formed—the eyes, ears, nose, hands, feet, abdominal organs, and numerous glands. Thus, at the end of12 two months, almost every structure and organ necessary to life is present in a rudimentary state.
By the close of the third month, witness the work of creation! From the blending of the two germ cells there has come forth a beautifully formed body (Fig. 1). True, it is but three and one half inches in length, but it is nevertheless a perfect body. About this time, the sex may be determined. The eyes, nose, ears, chin, arms and legs and even the fingers and toes may all be clearly distinguished.
A "jelly mass" at three months? No, by no means! No! Life and form and features are all there. It really has a face, whose features may easily be delineated.
In all my experience, I have yet to find the woman who wished to continue in her wicked and criminal intent after she had listened to this story of the creative development of the first three months of her "child enmothered."
During the next four months, which take us to the close of the seventh, rapid growth and farther development take place to the extent, that, should birth occur at that time, life may continue under proper conditions.
Everything is now nearing completion—only awaiting further growth, development, and strength—except some of the bone development, which takes place during the remaining two months. Growth is rapid, strength is doubled, and as the two hundred and seventy-three days draw to a close, everything has been completed. It has all taken place according to the laws of creation in an infinite way and with clock-like precision.
With the developmental growth of the product of conception, the uterus or room that had been particularly prepared for the "big reception" of the second week, has also grown to great dimensions. It fills almost the entire abdomen and as a result of the pressure against the diaphragm the breathing is somewhat embarrassed.
The door of this "room" has been closed by a special13 mechanism, while, in the fullness of time, Mother Nature begins the delicate work of opening the door, through whose portals passes out into the world the completed babe.
The authors feel that this discussion of, and protest against, abortions, should be accompanied by an appropriate consideration of the control of pregnancy. We are never going to eliminate the abortion curse of present-day civilization by merely preaching against it—warnings and denouncements alone will not suffice to remove the stain. Notwithstanding our feelings and convictions in this respect, we are also well aware of the fact that public sentiment is not now sufficiently ripe to welcome such a full and frank discussion of the subject of the prevention of conception as the authors would feel called upon to present; we are equally cognizant of the fact that existing postal regulations and other Federal laws are of such a character (at least capable of such interpretation) as possibly to render even the scientific and dignified consideration of such subjects entirely out of question.
In the preceding chapter we learned that when the two germ cells came together, there occurred a complete blending of two separate and distinct hereditary lines, reaching from the present away back into the dim and distant past. By the union of these two ancestral strains a new personality is formed, a new individual is created, with its own peculiar characteristics.
Probably none of the laboriously acquired accomplishments of the present generation can be directly—and as such—handed down to our children. What we are to be and what we will do in this world was largely determined by the laws of heredity by the time we were well started on our development experience en-utero during the third or fourth week of our prenatal existence, as outlined in a former chapter.
It is now generally accepted in scientific circles that acquired characteristics are not transmissible. Someone has aptly stated this truth by saying that "wooden heads are inherited, but wooden legs are not." This does not by any means imply that we do not have power and ability to fashion our careers and carve out our own destiny, within the possible bounds of our hereditary endowment and environmental surroundings. Heredity does determine our "capital stock," but our own efforts and acts determine the interest and increase which we may derive from our natural endowment. From the moment conception takes place—the very instant when the two sex cells meet and blend—then and there "the gates of heredity are forever closed." From that time on we are dealing with the problems15 of nutrition, development, education, and environment; therefore, so-called prenatal influence can have nothing whatever to do with heredity.
A father may have acquired great talent as a physician or a surgeon, in fact he may hold the chair of surgery in a medical college, but each of his children come into the world without the slightest knowledge of the subject, and, as far as direct and immediate heredity is concerned, will have to work just about as hard to master the subject as will the same average class of children whose parents were not surgeons. This must not be taken to mean that certain abilities and tendencies are not inheritable—for they are; but they are inherited through the parents—and not from them—directly. These transmitted characteristics are largely "stock" traits, and usually have long been present in the "ancestral strain."
A mother may sing and pray all through the nine months of expectancy, or she may weep and scold, or even curse. In neither case can she influence the spiritual or moral tendencies of her child and cause it, through supposed prenatal influence, to be born with criminal tendencies or to grow up a pious lad or become a devout minister. These tendencies and characteristics are all largely determined by the "depressors," "suppressors," and "determiners" which were present in the two microscopic and mosaic germ cells which united to start the embryo at the time of conception.
The child is destined to be born, endowed, and equipped with the mental, nervous, and physical powers which his line has fallen heir to all through the past ages. Down through the ages education, religion, environment, and other special influences have no doubt played a small part in influencing and determining hereditary characteristics; just as environment in the ages past changed the foot of the evolving horse from a flat, "cushiony" foot with many toes (much needed in the soft bog of his earlier existence) into the "hoof foot" of later days, when harder soil and necessity for greater fleetness, assisted by some sort of "selection" and "survival," con16spired to give us the foot of our modern horse, and this story is all plainly and serially told in the fossil and other remains found in our own hemisphere. It would appear that many, many generations of education and environment are required to influence markedly the established and settled train of heredity regarding any particular element or characteristic in any particular line or lines of hereditary tendencies.
There is probably more misinformation in the minds of the people on the subject of "maternal impressions" and "birthmarks" than any other scientific or medical subject. The popular belief that, if a pregnant woman should see an ugly sight or pass through some terrifying experience, in some mysterious way her unborn child would be "marked," deformed, or in some way show some blemish at birth, is a time-honored and ancient belief.
Such unscientific and unwarranted teaching has been handed down from mother to daughter through the ages, while the poor, misguided souls of expectant women have suffered untold remorse, heaped blame upon themselves, lived lives literally cursed with fear and dread—veritable slaves to superstition and bondage—all because of the simple fact that a certain percentage of all children born in this world have sustained some sort of an injury or "embryological accident" during the first days of fetal existence. For instance, take the common birthmark of a patch of reddened skin on the face, brow, or neck. As soon as the baby is born, the worried mother asks in anxious tones: "Doctor, is it all right, is it perfect, has it got any birthmarks?" On being told that the baby has a round, red patch on its left brow, the ever-ready statement of the mother comes forth: "Yes, I knew I'd mark it, I was picking berries one day about three months ago, and I ate and ate, until I suddenly remembered I might mark my baby, and before I knew what I was doing, I touched my brow and I just knew I had marked my baby." Do you know, reader, that that birthmark was present fully four months before she passed through that experience in the berry patch? And yet so worried17 and apprehensive has been the pregnant mother, that, although she can never successfully predict the "birthmarks" and blemishes of her child, nevertheless when these defects are disclosed at birth she is unfailingly able immediately to recall some extraordinary experience which she has carefully stored away in her memory and which, to her mind, most fully explains and accounts for the defect.
Is it much wonder that in the very early days of embryonic existence, during the hours of delicate cell division, indentation, outpushing, elongation, and sliding of young cells—is it much wonder, I repeat—that there occur a few malformations, blemishes, or other accidents which persist as "birthmarks?"
There are many factors which may enter into the production of birth-blemishes, deformities, monstrosities, etc. These influences are all governed by certain definite laws of cause and effect. A pre-existent systemic disease in the father, or a coexistent disorder in the mother, may be a leading factor. A mechanical injury, such as a sudden fall, a blow, or a kick, or certain kinds of prolonged pressure, not to mention restrictions and contractions of the maternal bony structures, may all possibly contribute something to these prenatal miscarriages of growth and development. Maternal or prenatal embryonic infections could bring about many sorts of birthmarks and malformations. These defects might also be caused by certain types of severe inflammatory disorders in the uterus during the early days of pregnancy.
The same factors that produce the accidents of embryology resulting in malformations or monstrosities in the human family, are also operative in the case of our lesser brethren of the animal kingdom, for monstrosities and birth-defects are very common among the lower animals, notwithstanding the fact that the animal mother probably does not "believe in birthmarks."
"It is a striking fact that during the nineteenth century, the teratologists, those who have scientifically investigated the causes of monstrosities and fetal morbid states, have almost18 without exception, rejected the theory of maternal impressions." Scientists and physicians are coming to recognize the fact that fears and frights do not in any way act as causes in the production of monstrosities and deformities. Let us seek forever to liberate all womankind from the common and harassing fear and the definite dread and worry that, because they failed to control themselves at the instant of some terrifying sight or experience, they were directly responsible for the misfortune of their abnormal offspring.
It should be remembered that there exists no direct connection whatsoever between the nervous system of the unborn child and the nervous system of the mother. The only physiological or embryological relationship is of a nutritional order, and even that is indirect and remote.
By the end of the third month, the "cocoon" attachment described in chapter two has disappeared; the fetus is slowly pushed away from the uterus which has so snugly held it for more than eleven weeks; while upon the exact site of its previous attachment the thickened uterine membrane undergoes a very interesting and important change—definite blood vessels begin to form—which begin indirectly to form contact with the maternal vessels, and thus it is that the placenta, or "after birth" is formed; and then, by means of the umbilical cord, nourishment from the mother's blood-stream is carried to the growing and rapidly developing child. In exchange for the nourishing stream of life-giving fluid by which growth and development take place, the embryo gives off its poisonous excretions which are carried back to the placenta, from which they are absorbed into the veinous circulation of the mother; so, while the mother does, through the process of nutrition, influence growth and development in the embryo, she is wholly unable to produce specific changes and such definite developmental errors as birthmarks and other deformities.
Just as truly as it would be impossible so to frighten a setting hen as to "mark" or otherwise influence the form or character of the chicks which would ultimately come forth from19 the eggs in her nest, it is just as truly impossible to frighten the pregnant mother and thereby influence the final developmental product of the human egg which is so securely tucked away in its uterine nest; for, when conception has occurred, the human embryo is just as truly an egg—fashioned and formed—as is the larger and shell-contained embryo of the chick which lies in the nest of the setting hen.
And so we are compelled to recognize the fact that there is little more danger to the unborn child when the mother is frightened than when the father is scared. The one contributes as much as the other to the general character of the child, while neither is to blame for development errors and defects.
Certain fears are suggested to children. For twenty years I lived under the delusion that I was terribly afraid of snakes—more so than any other human being; for I was told when a mere child that I had been "marked with the fear of snakes," that just two months before I saw the peep of day, my esteemed mother had been terrified by a snake. Everywhere I went, I announced to sympathizing and ofttimes mischievous friends, that "I was marked with the fear of snakes and must never be frightened with them." It is needless to add in passing, that I was teased and frightened all through my girlhood days. I was a veritable slave to the bondage of snake-fear. Everywhere I went I looked for my dreaded foe, expecting to sit on one, step on one, or to have one drop into my lap from the roof.
The day of deliverance came after marriage, when in a supreme effort to deliver me from the shackles of fear, the goodman of the house tenderly, but firmly, maneuvered a morning walk so that it halted in front of a large plate-glass window of the Snake Drug Store in San Francisco. Just back of this plate glass, and within eighteen inches of my very nose, were fifty-seven varieties of the reptiles, big and small, streaked and checkered, quiet and active. After much remonstrance and waiting, I came-to—gazed at the markings, beautiful in their20 exactness—while slowly the change of mind took place. Faith took the place of fear, calmness subdued panic, and I was wondrously delivered from the veritable bondage of a score of years. And so it is that the mother suffers and then the child suffers, ofttimes a living death, because of the superstition "I'm marked," while there is ever present the fear or dread that "something is going to happen, because I'm different from all other individuals—because 'I'm marked!'"
As soon as a woman discovers that she is pregnant, she should sit down and quietly think out the plan for the nine months of expectancy.
The cessation of the menses may come as a surprise to her, and for a while she is more or less confused; she must go over the whole situation and adjust future plans to fit in with this new and all important fact. From a large experience with maternity cases, I have reached the conclusion that the larger percentage of pregnancies do come as a surprise, and in many instances a complete change of program must be painstakingly thought out. This is especially true of the business woman, the professional woman, the busy club woman, or the active society woman.
Let me say to the woman who is pregnant for the first time, the experiences of the pregnant state should cause you no fear, worry, or anxiety. Giving birth to a baby is a perfectly natural, normal procedure, and if you are in reasonable health—if your physician tells you you are a fairly normal woman—then you can dismiss further thought of danger and go on your way rejoicing. For thousands of years maternity has been women's exclusive profession and no doubt will continue to be many ages hence.
By far the most important and the first thing to do is carefully to select the best physician your means will allow, and place yourself under his or her care. Your doctor will help you to plan wisely and intelligently during the waiting time, for physicians have learned from experience that the better22 care the pregnant woman receives, the easier will be her labor, and the more speedy and uneventful the recovery.
And now, we proceed to take up one by one the particular phases of the hygiene of pregnancy which touch the comfort, convenience, and health of both the mother and her unborn child.
At all times and under all circumstances the pregnant woman's clothing should be comfortable, suitable for the occasion, artistic, and practical. And to be thus beautifully clothed is to be as inconspicuous as is possible. Of all times, occasions, and conditions, that of pregnancy demands modesty in color, simplicity in style, together with long straight lines (Fig. 2). For the "going out" dress, select soft shades of brown, blue, wine, or dark green. Let the house dresses be simple, easy to launder, without constricting waist bands, of the one-piece type, in every way suitable for the work at hand. Under this outer dress, a princess petticoat should cover a specially designed maternity corset (if any corset at all be worn), to which is attached side hose-supporters. A support for the breasts may be worn if desired, it should be loose enough to allow perfect freedom in breathing.
The union suit may be of linen, silk, or cotton, with the weight suitable for the season. Stockings and shoes should be of a comfortable type, straight last, low or medium heel and at least as wide as the foot. There are two or three shoes on the market that are particularly good, whose arches are flexible, heels comfortable, straight last, and whose soles look very much like the lines of the foot unclothed. This style is particularly good during the maternity days. Painful feet are a great strain upon the general nervous system. Who of us has not seen women with strained, tense faces hobbling about in high-heeled, narrow-toed shoes? And if we followed them we would not only see tenseness and strain in the features of the face, but could hear outbursts of temper on the least provocation. Aching feet produce general irritability. If ease of body and calmness of spirit is desired, wear shoes that are comfortable, and the surprising part of it is that many of them are very good looking.

The long lines, so admirable for maternity wear are portrayed in this handsome afternoon costume. Tunic waist is made with shoulder yoke from which fullness hangs in fine plaiting with panel at back, front and under arms. The set in vest is of black-striped gold cloth trimmed with gold thread crochet buttons and with tiny waistcoat of black moire. Sleeves are of Georgette crepe. Loose adjustable girdle of black moire ribbon. Full skirt is attached on elastic to china silk underbodice. Material Crepe de chine or any other soft, clinging fabric.
24Toward the end of pregnancy ofttimes the feet swell, in which instance larger shoes should be worn in connection with the bandaging of the ankles and legs.
During the latter days of expectancy an abdominal supporter may be worn advantageously. Much of the backache and heaviness in the pelvis is entirely relieved by the supporting of the pendulous abdomen with a well-fitted binder. An ordinary piece of linen crash may be fitted properly by the taking in of darts at the lower front edge; or elastic linen, or silk binder may be secured; in fact, any binder that properly supports the abdomen will answer the purpose.
It should be within the means of every pregnant woman to have a neat, artistic out-door costume, for social, club and church occasions (Fig. 2). For no reason but illness should an expectant mother shut herself up in doors.
True men and true women hold the very highest esteem for the maternal state, and the opinion of all others matters not; so joyfully go forth to the club, social event, concert, or church; and to do this, you must have a well-designed, artistic dress. The material does not matter much, but the shade and style are important.
There are certain laws which govern the diet at all times; for instance, the man who digs ditches requires more of a certain element of food and more food in general, than does the man who digs thoughts out of his brain. The growing child requires somewhat different elements of food than does an adult. In other words, "The diet should suit the times, occasions, occupations, etc."
In the case of the expectant mother it should be remembered that the child gains nine-tenths of its weight after the fifth month of pregnancy, and it is, therefore, not necessary that a woman shall begin "eating for two" until after the fifth month. And since it is also true that the baby doubles its weight during the last eight weeks of pregnancy, it follows that25 then is the time when special attention must be given to the quantity as well as the quality of "mothers' food."
During the first five months, if the urine and blood-pressure are normal, the "lady in waiting" should follow her usual dietetic tastes and fancies so long as they do not distress or cause indigestion. Because of the additional work of the elimination of the fetal wastes, much water, seven or eight glasses a day, should be taken; while one of the meals—should there be three—may well consist largely of fruit. All of the vegetables may be enjoyed; salads with simple dressings and fruits may be eaten liberally. Of the breads, bran, whole wheat, or graham are far better for the bowels than the finer grain breads, or the hot breads.
Something fresh—raw—should be taken every day, such as lettuce, radishes, cabbage salad, and fresh fruits.
If the prospective mother is accustomed to the liberal use of meat, providing the blood-pressure and urine are normal, she may be able to indulge in meat once a day. Many physicians believe that the maternal woman should eat meat rather sparingly—from once a day to once or twice or three times a week.
Of the desserts, gelatine, junket, ice cream, sponge cake, and fruit are far better than the rich pastries, which never fail even in health to encourage indigestion and heart burn. The fruitades are all good. Candies and other sweets may be eaten in moderation. Alcohol should be avoided. Tea and coffee should be restricted, and in many cases abandoned. For many, two meals and a lunch of fruit or broth are better than three full meals. There is a continual and increased accumulation of waste matter which must be thrown off by the lungs, kidneys bowels, and skin; so that clogging of one channel of elimination makes more work for one or more of the other eliminative organs.
Sometimes the craving for food is excessive, and the desire to nibble between meals is quite troublesome. These unusual feelings should be controlled or ignored. A glass of orangeade will sometimes satisfy this unnatural craving. Save your appetite for meal time—for a good appetite means good digestion26 —all things equal. The woman who habitually eats between meals is the sluggish, constipated individual who needs to acquire self-control and learn self-mastery.
Water is the circulating medium of the body, from which the digestive secretions are formed, and by which the food is assimilated and distributed to individual cells. And, finally, water is the agent for dissolving and removing waste products from the body through the various eliminating organs. We literally live, think, and have our being, as it were, under water. The tiny cell creatures of our bodies, from the humble bile workers of the liver to the exalted thinking cells of the brain, all carry on their work submerged. Accordingly, the amount of water we drink each day, determines whether the liquids circulating through our tissues shall be pure, fresh, and life-giving, or stagnant, stale, and death-dealing.
Thirst is the expression of the nervous system, constituting a call for water, the same as hunger represents a call for food. Pure water, free from all foreign substances, is the best liquid with which to quench this thirst.
It is just as important to supply abundance of water for the proper bathing and cleansing of the internal parts of the body, as it is to wash and bathe the external skin frequently. The living tissues are just as literally soiled and dirtied by their life action and their poisonous excretions, as is the skin soiled by its excretions of sweat and poisonous solids. Thus the regular drinking of water is absolutely necessary to enable the body to enjoy its internal bath, and this internal cleansing is just as grateful and refreshing to the cells and tissues, as is the external bath to the nerves which exist in the skin.
The total amount of water necessary varies according to the nature of one's work, the amount of sweating from the skin, the moisture of the atmosphere, the amount of water in the food, etc. We believe the average person requires about eight glasses of liquid a day; that is, about two quarts. By the word "glass" we refer to the ordinary glass or goblet, two of which equal one pint. This amount of water should be27 increased, if anything, throughout pregnancy; while, during the later months, the amount of water taken each day should be at least doubled.
In the condemnation of so-called artificial beverages, an exception should be made of the fruit juices. The fresh, unfermented juices of various fruits come very near being pure, distilled water, as they consist of only a little fruit sugar and acid, together with small amounts of flavoring and coloring substances, dissolved in pure water. None of these substances contained in pure fruit juice needs to be digested.
Lemonade not too sweet, and taken in moderate quantities, is certainly a beverage free from objection when used by the average pregnant woman. Unripe or overripe fruits frequently cause bowel disturbances; as also do the millions of germs which lurk upon the outside of fruits, and which find their way into the stomach and bowels when these fruits are eaten raw without washing or paring. Otherwise, the juices of fruits and melons are wholesome food beverages when consumed in moderation.
It should be the regular practice of every expectant mother to spend a portion of each day in agreeable, suitable exercise or physical work of some description. This exercise will be far more beneficial if it can be taken in the open air. The weather and the strength of the patient must be taken into consideration and the necessary modifications of the daily exercise should be made.
An expectant mother living in the city and enjoying the average health and strength, should engage in such agreeable exercise as the raising of flowers, the training of vines, with brisk walks in the fresh air. As much time as possible should be spent in the parks.
The rural "mother in waiting," may do light gardening, raising of chickens, or pigeons, training of vines, or other outdoor work she may enjoy.
No matter what kind of weather prevails, a daily brisk walk should be taken, out of doors, on the porch or in a room with28 open windows. A daily sweat, as well as the daily prayer, is good for the well-being of the expectant mother. All forms of light housework are commendable. Keep out of crowds. Spend more time in the parks than in the department stores. An occasional evening at the concert or theater is diversion and harmless provided the ventilation is good. Such exercises as horseback riding, bicycling, dancing, driving over rough roads, lifting and straining of any kind, and all other forms of fatiguing exercise should be avoided.
Rest and relaxation are quite necessary for men and women even in the best of health. A kind providence has arranged that we spend a large portion of our time resting, and sleeping. In addition to unbroken rest at night it is well for the prospective mother quietly to withdraw from the family circle, when the first signs of fatigue begin to appear, and indulge in a little rest, before she gets into a state of nervousness—where nerves twitch and she becomes irritable.
A mother who has borne six children, who has had little domestic help, and who yet retains her youthful appearance and energy, thinks her present condition due to the fact that while carrying and nursing her babies she never permitted herself to reach that stage of exhaustion where her nerves twitched, her voice shrilled, and she became irritable. She made it a practice to drop her work when these symptoms began to appear, and to seek the sanctuary of a quiet room apart from her family, if only for ten or fifteen minutes. And, most important, from the very start she trained her household to respect her right thus to draw apart.
I have told many women whose household duties press hard: "Your husband would rather see a cold lunch on the table, or 'go out' for dinner, while his wife rested, smiling and happy, than to have a most sumptuous meal spread before him and the wife tired, and fretful." Every woman should make it the rule of her life to stop just this side of the outburst of words, and lie down long enough, breathing deeply, to calm the spirit.29
"With all persons plenty of fresh air, night and day, is indispensable to health, and to none more than the pregnant woman. She should sleep with the windows open, or out of doors, at all seasons of the year; of course, making due allowance for the severity of the winters in the North. It is not only necessary to provide for the adequate ventilation of sleeping-rooms, but also for that of the living-rooms of the house.
Many persons, who are quite particular to open wide the windows of the bedrooms, forget that the other rooms need it quite as much. All the rooms of the house which are occupied should be thoroughly ventilated by throwing doors and windows open every morning; at night when the family is assembled the air must be changed now and then or it will become unfit for human lungs."
Men and women are outdoor animals. They were made to live in a garden, not a house. Remember that each person requires one cubic foot of fresh air every second. Don't allow the temperature of living-rooms, during the winter season, to go above sixty-eight degrees. If your home has no system of ventilation, open wide the windows and doors several times a day and enjoy the blessings of a thorough-going flushing with fresh air.
Oxygen is the vital fire of life. Our food, however well digested and assimilated, is just as useless to the body without oxygen, as coal is to the furnace without air. It is equally important to keep up the proper degree of moisture in the air of the living-rooms.
Bathing is made necessary by the clothes we wear and by our indoor life. If the skin were daily exposed to sunshine and fresh air, it would seldom be necessary to bathe. The neglect of regular bathing results in overworking the liver and kidneys, and debilitates the skin. Regular bathing—ofttimes sweating baths—is very essential to the hygiene of pregnancy.30
The neutral bath (97 F.) is excellent to quiet the nerves and induce sleep. Morning bathing is an exceedingly valuable practice. If properly taken before breakfast or midway between breakfast and lunch, it is found to be refreshing and tonic in nature. The feet should be in warm water, the application of cold should be short and vigorous. A rough mit dipped in cold water, rubbed over the body until the skin is pink, is a splendid tonic.
Warm cleansing baths should be taken twice a week at night. There is no good reason for the use of the vaginal douche during pregnancy.
Because the mother's system is drained of the lime salts which aid in building up the bones of the child, along with other metabolic changes which cause the retention of certain acids which ofttimes affect the teeth, they should be frequently examined and carefully guarded. Severe dental work should be avoided, but all cavities should receive temporary fillings while the teeth are kept free from deposits.
As a preventive to this tendency of the teeth to decay, a simple mouth wash of one of the following may be used after meals:
Any one to be dissolved in a glass of water.
Beginning with the second voiding of urine after rising on the morning of the day you are to save the specimen, save all that is passed during the following twenty-four hours, including the first voiding on the second morning. Measure carefully the total quantity passed in the twenty-four hours. Shake thoroughly so that all the sediment will be mixed, and immediately after shaking take out eight ounces or thereabouts for delivery to the physician the same forenoon. The following items31 should be noted, and this memoranda should accompany the specimen:
1. Patient's name.
2. Address.
3. This specimen was taken from a twenty-four hour voiding of urine, which began at .... a. m. ...., and ended at .... a. m. ....
4. The total quantity voided during this twenty-four hours was .... pints.
This specimen should reach the laboratory by ten o'clock the same morning.
It is of utmost importance the specimen should be taken to your physician every two weeks, and oftener if conditions indicate it. Take it yourself at the appointed time.
Owing to the increasing pressure exerted upon the intestines, most expectant mothers experience a tendency to sluggish bowels and constipation. This unpleasant symptom is usually increased during the later months.
In the first place, a definite time must be selected for bowel action. It may ofttimes be necessary, and it is far less harmful, to insert a glycerine suppository into the rectum, than to get into the enema habit. The injection of a large quantity of water into the lower bowel will mechanically empty it; but the effects are atonic and depressing as regards future action.
Before we take up the advisability of taking laxatives let us consider what foods will aid in combating constipation. The following list of foods are laxative in their action and will be found helpful in overcoming the constipation so often associated with pregnancy:
1. All forms of sugar, especially fruit sugar, honey, syrup, and malt. All the concentrated fruit juices. Sweet fruits, such as figs, raisins, prunes, fruit jellies, etc.
2. All sour fruits, and fruit acids: Apples, grapes, gooseberries, grape fruit, currants, plums, and tomatoes.
3. Fruit juices, especially from sour fruits: Grape juice, lemonade, fruit soup, etc.32
4. All foods high in fat: Butter, cream, eggs, eggnog, ripe olives, olive oil, nuts—especially pecans, brazil nuts, and pine nuts.
5. Buttermilk and koumiss.
6. All foods rich in cellulose: Wheat flakes, asparagus, cauliflower, spinach, sweet potatoes, green corn and popcorn, graham flour, oatmeal foods, whole-wheat preparations, bran bread, apples, blackberries, cherries, cranberries, melons, oranges, peaches, pineapples, plums, whortleberries, raw cabbage, celery, greens, lettuce, onions, parsnips, turnips, lima beans, and peanuts.
White bread should be tabooed, and in its place a well-made bran bread should be used. Two recipes for bran bread follow, one sweetened and containing fruit, the other unsweetened:
1. Two eggs, beaten separately; three-fourths cup of molasses, plus one round teaspoon of soda; one cup of sour cream; one cup of sultana seedless raisins; one cup of wheat flour, plus one heaping teaspoon baking powder; two cups of bran; stir well and bake one hour.
2. One cup of cooking molasses; one teaspoon of soda; one small teaspoon of salt, one pint of sour milk or buttermilk, one quart of bran, one pint of flour. Stir well, and bake for one hour in a very slow oven. It may be baked in loaf, or in gem pans, as preferred. The bread should be moist and tender, and may be eaten freely, day after day, and is quite sure to have a salutary effect if used persistently.
The drinking of one-half glass of cold water on rising in the morning often aids in keeping the bowels active. Of the laxative drugs which may be used at such a time, cascara sagrada and senna are among the least harmful. Two recipes of senna preparation follow, and may be tried in obstinate cases:
1. Senna Prunes. Place an ounce of senna leaves in a jar and pour over them a quart of boiling water. After allowing them to stand for two hours strain, and to the clear liquid add a pound of well-washed prunes. Let them soak over night. In the morning cook until tender in the same water, sweetening33 with two tablespoons of brown sugar. Both the fruit and the sirup are laxative. Begin by eating a half-dozen of the prunes with sirup at night, and increase or decrease the amount as may be needed.
2. Senna with prunes and figs. This recipe does not call for cooking. Take a pound of dried figs and a pound of dried prunes, wash well. Remove the stones from the prunes and if very dry soak for an hour. Then put both fruits through the meat chopper, adding two ounces of finely powdered senna leaves. Stir into this mixture two tablespoons of molasses to bind it together, the result being a thick paste. Begin by eating at bedtime an amount equal to the size of an egg, and increase or decrease as may be necessary. Keep the paste tightly covered in a glass jar in a cool place. If the senna is distasteful a smaller quantity may be used at first.
The breasts are usually neglected during the months of pregnancy, and as a result complications occur after the baby comes which cause no end of discomfort to the mother. If, during the pregnancy, the breasts are washed daily with liquid soap and cold water, and rubbed increasingly until all sensitiveness has disappeared, they may be toughened to the extent that no pain whatsoever is experienced by the mother when the babe begins to nurse. During the last month of pregnancy a solution of tannin upon a piece of cotton may be applied after the usual vigorous bathing. If the nipples are retracted they should be massaged until visible results are attained.
Keep the mind occupied with normal, useful, and healthy thoughts. Listen to no tales of woe. Stay away from the neighborhood auntie dolefuls. Keep yourself happy and free from all worry, care, and anxiety.
"Put no faith in fables of cravings, markings, signs, or superstitions. They are all unfounded vagaries of ignorant old women and will not bear investigation."
Don't take drugs for worry and sleeplessness. Take a bath.34
The secret of deliverance from worrying is self-control. Minimize your difficulties. Cultivate faith and trust.
The conditions which favor sound sleep are: Quiet, mental peace, pure blood, good digestion, fresh air (the colder the better), physical weariness (but not fatigue), mental weariness (but not worry).
When tempted to borrow trouble, when harassed by fictitious worries, remember the old man who had passed through many troubles, most of which never happened. Train the mind to think positive thoughts. Replace worry-thought with an opposite thought which will occupy the mind and enthuse the soul. Drive out fear-thought by exercising faith-thought. Cultivate the art of living with yourself as you are, and with the world as it is. Learn the art of living easily. Associate with children and learn how to forget the vexing trifles of everyday life.
There is something decidedly wrong with one's nerves when everybody is constantly "getting on them." They are either highly diseased or abnormally sensitive. Every woman is a slave to every other that annoys her.
Fear is capable of so disarranging the circulation as to contribute to the elevation of blood-pressure—which will be more fully considered in a later chapter.
It is the purpose of this chapter to take up the various complications which may appear in the course of an otherwise normal pregnancy, and offer advice appropriate for their management.
About one-half of the expectant mothers that come under our care and observation, experience varying degrees of nausea or "morning sickness." This troublesome symptom makes its appearance usually about the fourth week of pregnancy and lasts from six to eight weeks.
On attempting to rise from the bed, there is an uncomfortably warm feeling in the stomach followed by a welling up into the throat of a warmish, brackish tasting liquid which causes the patient to hasten to rid herself of it; or, as she rides on the train, on the street cars, in a carriage or automobile, she frequently senses the same unpleasant and nauseating symptoms during the second and third months of pregnancy. Normally, this uncomfortable symptom quite disappears by the end of the third month. A number of remedies have been suggested for it, but that which seems to help one, gives little or no relief to another; we therefore mention a variety of remedies which may be tried.
First and most important of all remedies—is to keep the bowels open. Sluggishness of the intestinal tract greatly increases the tendency to dizziness and nausea. During the attack, it is advisable not to attempt to brush the teeth, gargle, or even drink cold water. While you are yet lying down, the maid or the goodman of the house should bring to you a piece36 of dry, buttered toast, a lettuce sandwich with a bit of lemon juice, or perhaps a cup of hot milk or hot malted milk. Coffee helps to raise the blood-pressure, and all articles of diet that tend to raise the blood-pressure are best avoided during pregnancy. A cup of cocoa may be tried, but, as a rule, women at this time do not relish anything sweet. Oftentimes a salted pretzel is just the thing, or a salted wafer will greatly help. Remain in bed from one-half to one hour and then rise very slowly. There should be plenty of fresh air in the room, as remaining in overheated places is quite likely to produce a feeling of sickness at the stomach.
When the attack comes on during a train ride, open the window and breathe deeply, this, with the aid of a clove or the tasting of a bit of lemon, will usually give relief. In extreme instances the patient should lie down flatly on the back, with the eyelids closed. Go to the rear of the street car, so that you can get off quickly if necessity demands; breathe deeply of the air; resort to the use of cloves or lemons; and thus by many and varied methods will the expectant mother be enabled to continue her journey or finish her shopping errand. We would suggest that, as far as possible, walking should be substituted for riding. I have never heard of a woman being troubled with nausea while walking in the parks, on shady streets, along the country road, or on the beach.
Of the medicines prescribed for "morning sickness" and the nausea of pregnancy, cerium oxalate taken three times a day in doses of five grains each, is probably one of the best.
The persistent or pernicious vomiting which continues on through pregnancy will be spoken of later.
Acid eructations are spoken of as "heartburn," and are occasioned by the increased activity of the acid making glands of the stomach. Under certain conditions this acid content of the stomach is regurgitated back into the throat and even belched up into the mouth. In this condition it is well to avoid most acid fruits. Ice cream and other frozen desserts are beneficial. The lowered temperature of cold foods depresses37 the activity of the acid glands, as also does the fats of the cream, while protein food substances such as white of egg, cheese, and lean meat, help by combining with the excess of acid present in the stomach. Buttermilk or the prepared lactic acid milk, if taken very cold, is often helpful, notwithstanding it is an acid substance, in connection with the dietetic management of heartburn. If the acid eructations be troublesome between the meals, the taking of calcined magnesia (one round teaspoon in a glass of cold water), or, one-half teaspoon of common baking soda in a glass of water, will afford immediate and temporary relief. Simply nibbling a little from a block of magnesia will often give instant relief. These alkalines effectively neutralize the mischievous acids which cause the so-called "heartburn."
The flexing or bending forward of the gravid uterus, by making pressure on the bladder, sets up more or less irritation and consequent disturbance of the urinary function. The capacity of the bladder is actually diminished, and this produces frequent urination. There is usually no pain connected with this annoying symptom—the chief discomfort is the frequent getting up at night. This inconvenience may be lessened by drinking less water after six p. m. These bladder disturbances are most marked in the earlier months, and gradually disappear as the uterus raises higher up into the abdomen; although this symptom may reappear in the last two weeks, as the head descends downward on its outward journey.
Should the urine at any time become highly colored, take a specimen to your physician at once. Twenty-four hour specimens of urine should be taken by the patient to her physician every two weeks. Do not send it—take it.
While leucorrhea is an unusual complication of pregnancy, it is often very troublesome and sometimes irritating. Do not take a vaginal douche unless it has been ordered by your physician, and even then make sure that the force of the flow of38 water is very gentle. The bag of the fountain syringe should be hung only about one foot above the hips. Soap and water used externally, followed by vaseline or zinc ointment, will usually relieve the accompanying irritation.
In the third chapter attention was called to the formation of the placenta or "after birth," on the site of the attachment of the cocoon embryo. At this particular time of the pushing away of the embryo from the uterine wall, one of the accidents of pregnancy occurs, in which the embryo becomes completely detached and starts to escape from the uterus, accompanied by varying degrees of pain and hemorrhage. The symptoms of this threatened abortion are:
The approach of the calendar date of the third month of pregnancy should be watched for, and all work of a strenuous nature studiously avoided; while at the first signs of the backache or any unusual symptom, the expectant mother should immediately go to bed and send for the physician. One patient who had aborted on four different occasions was able to pass this danger period by adhering to a rigid program of prevention during her fifth pregnancy. Two weeks before the third month arrived she discontinued her teaching and went to bed. She remained there four weeks, thus running over into the middle of the following month. Gradually, she resumed her duties of teaching, carried her precious bundle of life to full term, and is now the proud and happy mother of a splendid baby girl.
Should abortion seem imminent, from one-eighth to one-fourth of a grain of morphine sulphate will greatly reduce all uterine contractions, and this, with the general quieting effect on the whole system, will usually suffice to prevent an abortion. The patient should quietly remain in bed from three days to one week.39
If the abortion takes place—if a clot accompanied by hemorrhage is passed—save everything, lie in bed very quietly and send for your physician at once; and when he does arrive, be content if he does not make an internal examination at once, for if he should there is more or less danger of infection. And I repeat—throw nothing away—burn nothing up, save everything that passes until your physician has carefully examined it.
Sudden or severe pains in the abdomen should be reported at once to your physician, while you should immediately go to bed and quietly remain there until you receive further instruction from your doctor when he calls.
In the later stages of pregnancy any appearance of blood should likewise be noted and reported without delay. These symptoms may not always be serious, but they are also associated with grave complications, and should, therefore, be given prompt attention.
Abortion is a term used to designate the loss of the embryo prior to or at the third month. Miscarriage applies to the expulsion of the fetus or emptying of the uterus after the third month. It is possible for a miscarriage to occur anytime during the interim between the fourth and ninth months. After the uneventful passing of the third month, if an accident threatens, we instruct the mother to remain quietly in bed three to five days at the calendar date comparable with each menstrual period; and as she approaches the seventh month, we adjure her to be unusually careful and prudent.
The causes of miscarriages are many: Disease of the embryo, imperfect fetal development, some constitutional disease of the mother, a faulty position of the uterus, or it may result from something unusual about the lining of the uterus such as an endometritis—an inflammation of the mucus membrane.
Expectant mothers who manifest symptoms of a threatened miscarriage should studiously avoid such exercises as climbing, riding, skating, tennis, golf, dancing, rough carriage or auto40mobile riding, and such taxing labor as sweeping, lifting, washing, running the sewing machine, window cleaning, the hanging of pictures, draperies, etc.
Within reason, a pregnant mother should follow her natural appetite and satisfy her dietetic longings. Should she desire unusual articles of food, as far as possible she should have them. The idea has long prevailed that if the mother does not get what her longing soul supremely desires, that the on-coming baby is going to cry and cry until it is given what the mother wanted with all her heart and did not get. Such an idea is the very quintessence of folly and the personification of foolishness and superstition.
Many a precious babe has suffered as a victim of this notion of "craving" and "marking." One mother gave her baby a huge mouthful of under-ripe banana because "she knew that was just what he wanted, because, when pregnant, she had craved and craved bananas and for some reason or another she did not get them." The soft, smooth piece of banana slipped down the baby's throat—on into the stomach and intestines—caused intestinal obstruction and finally the end came; and we registered one more victim to the fallacies of fear and the superstitious belief in "cravings" and "markings." Occasionally some cravings are unusual and freakish, for instance, egg shells, leather, candles, chalk, and other abnormal tastes are developed. Of these we have only to say, "Rise above them, become mistress of the situation and change your longings." If such abnormal cravings come to you in the kitchen, don your bonnet and go at once out of doors and take a walk. Don't be foolish just because somebody told you foolish stories about these things.
Bowel hygiene is an important part of the management of pregnancy. Constipation often proves to be very troublesome. In another chapter this subject is treated at some length. Here, we pause only long enough to say that habit has much to do41 with this difficulty. A regular time should be set apart each day for attending to this important matter.
Of all the maladies that the human family falls heir to, hemorrhoids are among the commonest and, we may add, the most neglected. Any woman who enters pregnancy, suffering from hemorrhoids, is going to have her full share of suffering and pain before she has finished with her labors. Taken early, they may be greatly helped, if not entirely relieved, by the daily use of the medicated suppository (See Appendix). The bowel movements should never be allowed to become hard, the dietetic advice of another chapter should be carefully followed and the oil enema, as described in the appendix, should be used if necessary. For immediate relief, hot witch-hazel compresses may be applied; or, in the case of badly protruding piles, the patient should immerse the body in a warm bath and by the liberal use of vaseline they can usually be replaced. The physician should be called and he will advise any further treatment the case may require.
Varicose veins or the distension of the surface veins of the legs are very common among women in general and pregnant women in particular. The legs should be elevated whenever the patient sits, while in bad cases they should be bandaged while standing. There are many elastic surgical stockings on the market today that, if put on before rising in the morning, will give much relief and comfort all during the day. Any large medical house or physician's supply house can furnish them according to your measurements—which should be taken before getting out of bed in the morning. These measurements are taken according to instructions and usually are of the instep, ankle, calf of leg, length of ankle to knee, etc.
Cramps are sharp, exceedingly painful muscular spasms occurring in the muscles of the calf of the leg, the toes, etc. The42 expectant mother in the later months of pregnancy awkwardly turns in bed, is suddenly awakened and without a moment's warning, is seized with a most excruciating pain in her leg or toe. The most effectual treatment for these cramps is quickly to apply a very cold object to the cramping muscle. Extremes of either heat or cold usually relieve as well as the vigorous grasping or kneading of the muscle. A hot foot bath on going to bed will often prevent an attack. A long walk in the latter months of pregnancy should invariably be followed by a short hot bath or a foot bath. Many attacks may be avoided by this procedure.
All swellings should be taken seriously by the pregnant mother to this extent, that she save a twenty-four hour specimen of urine and that she personally take it to her physician, with a report of her "swellings." This symptom may or may not indicate kidney complications. The blood-pressure together with chemical and microscopical analysis of the urine will determine the cause.
Slight swelling of the feet is often physiological and is due to pressure of the heavily weighted uterus upon the returning veins of the legs. The progress of the veinous blood is somewhat impeded, hence the accumulation of lymph in the tissues of the legs, ankles, and feet.
Never allow yourself to guess as to the cause of swellings, always take urine to the physician and allow him definitely to ascertain the true cause. All tight bands of the waist and knee garters must be discarded at this time. The same general treatment suggested for varicose veins holds here.
The enlargement of the thyroid gland—goitre—is physiological during pregnancy, and is believed to be caused by the throwing into the maternal blood stream of special protein substances derived from the fetus. As just stated, this is more or less physiological, will usually pass away after the babe is born, and, therefore, need give the mother no particular con43cern. Tight neck bands should be replaced by low, comfortable ones. The bowels should move freely every day, and water drinking be increased as well as sweating of the skin encouraged by a short, hot bath, followed by the dry blanket pack, while the head is kept cool by compresses wrung from cold water. In this manner the elimination of these poisons is increased through both the skin and the kidneys.
The backache of the later months of expectancy is very annoying and often spoils an otherwise restful night's sleep. This is probably also a pressure symptom, if the physician's analysis of the urine proves that the kidneys are not at fault. If you have electric lights in the home, a very useful contrivance can be made which will give you great relief. The light end of an extension cord, five to seven feet in length, is soldered into the center of the bottom of a bright, pressed tin pail about twelve inches in diameter at the top and nine or ten inches deep. With the bail removed, screw in a sixteen or thirty-two candle power bulb and attach the extension cord to a nearby44 wall or ceiling socket. This arrangement supplies radiant heat and is called a photophore (See Fig. 3). Apply this twofold remedial agent—light and heat combined—to the painful back (underneath the bed clothing) and our restless mother will go to sleep very quickly. This may safely be used as often and as long as desired.
Persistent, prolonged, and very much aggravated cases of morning sickness are termed pernicious vomiting. The patient emaciates because of the lack of ability to keep food long enough to receive any benefits therefrom.
In treating these cases the sufferer should be put to bed in a room with many open windows, or, if the weather permit, should be out of doors on a comfortable cot. She should remain in bed one hour before the meal is served and from one to three hours afterward. The mind should be diverted from her condition by good reading, friends, or other amusements. The utmost care and tact should be used in the preparation of her food, and art should be manifested in the daintiness of the tray, etc. We found one mother was nauseated even at the sight of her tray and so we planned a call that should bring us to her home at the meal hour. The tray came in with the attendant in unkempt attire, who said, as she placed it carelessly down on a much-loved book our patient had been reading: "I heard you say you liked vegetable soup so I brought you a big bowl full." As I gazed at the tray, I saw a large, thick, gravy bowl running over with the soup. I usually like vegetable soup, but at the sight of that sloppy looking bowl—well, I thought I should never care for it again.
After installing a new maid who had a sense of service and daintiness, and who took real pleasure in the selection of the dishes for the tray, as well as the quality and quantity of food served in them, our patient made speedy recovery, went on to full term and became a happy mother.
There is no doubt that the mind has very much to do with this vexing complication of pregnancy. One mother immediately stopped vomiting everything she ate when told by her45 husband that "the doctor said he was coming in the morning to take you away from me to the hospital if you didn't stop vomiting." Everything known should be tried for the relief of these patients and in extreme cases, when the mother's life is endangered, pregnancy should be terminated.
The neutral full bath, temperature 97 F., maintained for twenty minutes to one-half hour, should be taken just on going to bed. The patient must not talk—must rest in the bath—absolutely quiet. The causes of insomnia should be determined if possible, and proper measures employed to remove them. They may consist of backache, cramps, frequent urination, pressure of the uterus on the diaphragm or pressure against the sides of the abdomen. The bed should be large, thus giving the patient ample room to roll about.
The following procedures may be tried in an effort to relieve the sleeplessness:
Rubbing of the spine, alcohol or witch-hazel rubbing of the entire body, the neutral bath, or the application of the electric photophore—described a few pages back—may be made to the painful part. Do not resort to drugs, unless you are directed to do so by your physician.
Headaches should not be allowed to continue unobserved by the attending physician. Measure the daily output of urine, which should be at least three pints or two quarts. In case of daily or frequent headaches, notify your physician at once and take a twenty-four hour specimen of urine to him. Headache is an early symptom of retained poisons and if early reported to the physician quick relief can be given the patient and often severe kidney complications be avoided by the proper administration of early sweating procedures. Water drinking should be increased to two quarts (about ten glasses) a day. Less food and more water are the usual indications in the headaches of pregnancy.46
Blood-pressure is called high when the systolic pressure registers above 150 to 160 millimeters of mercury. Pressure above 165 should be taken seriously and the patient should keep in close touch with her physician. Tri-weekly examinations of the urine should be made, while eliminating baths should be promptly instituted. The subject of blood-pressure in relation to pregnancy will be fully dealt with in the next chapter—in connection with toxemia, eclampsia, etc.
At the close of the preceding chapter on the complications of pregnancy, brief mention was made of blood-pressure as a possible source of anxiety. This chapter will be devoted to a further discussion of the subjects of toxemia, eclampsia, convulsions, and especially blood-pressure—in connection with other leading symptoms of these serious complications of pregnancy.
In a former chapter we learned that the developing child nearly doubled its weight in the last two months of pregnancy. As the child grows, its metabolic waste matter is greatly increased, while all these poisonous substances must finally be eliminated by the mother. Now, the mother's waste matter is of itself considerably increased; and so, if the kidneys, the liver, and the skin are already over-taxed in their work of normal elimination—if they are already doing their full quota of work—we can readily see that the additional waste matter of the unborn child will throw much extra work on the already overworked eliminative organs, and this results in a condition of toxemia. Certain symptoms accompany this state of constitutional poisoning or auto-intoxication—the chief of which are:
Any one of these symptoms may or may not indicate toxemia; but it should be reported at once to the attending physician. In the presence of one or more of these symptoms an expectant mother is always safe, while awaiting the physician's advice, in carrying out the following program:
This serious complication of the last weeks of pregnancy demands immediate attention. They may almost invariably be avoided if the blood-pressure and the urine are studiously watched during the latter part of the expectant period.
If you are unable to get your physician at once, the following treatment should be administered immediately.
1. A hot colonic flushing (See Appendix).
2. A hot bath followed by the hot blanket pack (See Appendix).
3. One drop of croton oil on a bit of sugar may be placed on the back of the tongue.
4. Chloroform may be administered, provided a competent nurse or other medical person is present.
The appearance of convulsions which have been preceded by one or more of the symptoms noted under the head of "toxemia," indicates that the patient has become so profoundly intoxicated and poisoned by the accumulating toxins, that the lives of both mother and child are jeopardized by threatened eclampsia. At such a time, the attending physician will immediately set about to bring on labor, and thus seek to empty the uterus at the earliest possible moment.
Since toxemia (eclampsia) is one of the complications of pregnancy most to be dreaded, it is fortunate that it almost invariably exhibits early danger signals which, if recognized and heeded, would enable the patient and physician to initiate 49proper measures to avert danger and escape the threatened disaster. The presence of this toxic danger is indicated by the persistent presence of the following three symptoms:
Of course, albumin will probably appear in the urine along with the casts, but it is the continued appearance of the casts that is of more importance as a danger signal. Albumin is quite common in the urine of the expectant mother, but casts—long continued—suggest trouble. Headache as an indicator of toxemia is of special significance when coupled with the other two cardinal symptoms of eclampsia—urinary casts and increasing high blood-pressure. Therefore, the necessity for frequent urinary tests and blood-pressure examinations during the last weeks of pregnancy—especially, if the patient has suffered from headaches and has been running albumin in the urine.
Blood-pressure is a term used to indicate the actual pressure of the blood stream against the walls of the blood vessels. The blood-pressure machine tells us the same story about our circulatory mechanism, that a steam gauge does about a high-pressure boiler (See Fig. 4). The normal blood-pressure varies according to the age of the patient. For instance, the normal pressure of a young person, say up to twenty years of age, runs from 100 to 120 millimeters of mercury; and then, as the age advances, the blood-pressure increases in direct ratio; for every two years additional age the blood-pressure increases about one point—one millimeter.
The average pregnant woman starts in her pregnancy with a blood-pressure of say, 125 millimeters, but as pressure symptoms increase, and as constipation manifests itself, and as the circulating fluids are further burdened with the toxins which are eliminated from the child, the blood-pressure normally increases to about 140 mm., and later, possibly to 150 mm.50 If the pressure goes no higher, we are not alarmed, for we have come to recognize a blood-pressure of 140 as about the normal pressure of the pregnant woman.
There are a number of factors which enter into the raising of the blood-pressure. For instance, at any time during the pregnancy, if the eliminative organs of the mother are doing inefficient work, if she falls a victim to a torpid liver, diseased kidneys, decreased skin elimination, or sluggish bowels, then, with the added and extra excretions from the child, there is superimposed upon the mother far more than the normal amount of eliminative work—and then, because of improper and incomplete elimination, the blood-pressure is increasingly raised.
This whole subject can best be illustrated by relating a story, the actual experience of Mrs. A. This patient came to the office with a history of Bright's disease (albumin and casts in the urine), and chronic appendicitis. While treating her for the kidney condition, preparatory to an operation for the removal of the troublesome appendix—in the very midst of this treatment—she became pregnant, and great indeed was our dismay. We entertained little hope of getting both the mother and child safely through. Frequent examination of urine was instituted, the albumin did not increase and the blood-pressure remained at normal—about 124 mm. She paid weekly or bi-weekly visits to the office and carefully followed the regime outlined. She drank abundantly of water and strictly followed the dietary prescribed. Weeks and months passed uneventful, until we approached the last six weeks of pregnancy, and then we found to our surprise one day that the blood-pressure had made a sudden jump up to 175 mm., while the urine revealed the presence of numerous casts and albumin—in the meantime the albumin had entirely disappeared. There were also other urinary findings which showed that the liver was not doing its share in the work of burning up certain poisons.
In her home we began the following program: Every day51 we had her placed in a bathtub of hot water, keeping cold cloths upon her brow, face and neck, and then, by increasing the temperature of the bath, we produced a very profuse perspiration. She was taken out of this bath and wrapped in blankets, thus continuing the sweat. All meat, baked beans, and such foods as macaroni and other articles containing a high per cent of protein were largely eliminated from her diet. At times she did not even eat bread. Her chief diet was fruit, vegetables, and simple salads, and yet the albumin and casts continued to increase in the urine and the blood-pressure climbed up to 190 mm.
As we approached the last two weeks of pregnancy, this little woman was taken to the hospital and systematic daily treatment with sweating procedures was begun. Among other things, she had a daily electric light bath. After each of these baths she was wrapped in blankets and the sweating continued for some time. Careful estimations of albumin were made daily and the blood-pressure findings noted three times a day. During the last week of pregnancy she lived on oranges and grapes. Day by day she was watched until the eventful hour arrived. She went into the delivery room and gave birth to a perfectly normal child. The albumin and casts quickly cleared up, the blood-pressure lowered, and today the little woman is a fond mother of a beautiful baby boy.
It is hard to estimate what might have taken place had not her elimination been stimulated. The blood-pressure was our guide. Had the albumin (without casts) appeared in the latter weeks of pregnancy with a blood-pressure of 140 or 150 mm., we would not have become excited, for the reason that in every normal pregnancy there is often present a trace of albumin in the latter weeks; but when the blood-pressure jumped to 170 or 190, then we knew that toxemia—eclampsia—convulsions—were imminent. So we have in recent years, come to look upon the blood-pressure as an exceedingly important factor—as an infallible indicator of approaching trouble—as a red signal light at the precipice or the point of danger; and it not only warns us of the danger, but it tells us about how near the boilers are to the bursting point. The glassy eye, the head52ache, the full bounding pulse and the blurring of vision, are all symptoms accompanying this high blood-pressure, so that in these enlightened days no practitioner can count himself worthy the name, or in any way fit to carry a pregnant woman through the months of waiting, unless he sees, appreciates, and understands the value of blood-pressure findings in pregnancy.
Two months before baby is to arrive, the expectant mother should pay particular attention to the conservation of her strength. The woman who is compelled to leave her home for the factory, the laundry, the office, or other place of employment, should stop work during these last two or three months. The active club woman should pass the burdens on to others, and the woman of leisure should withdraw from active social life with its varied obligations. During the final weeks of pregnancy, the prospective mother needs the same hygienic care regarding fresh air, exercise, diet, and water drinking, as outlined in a former chapter.
As the gravid uterus rises higher in the abdomen, increased pressure is exerted on the stomach, the lungs, and upon the nerve centers of the back; and it is because of this situation, that the duties and obligations of the prospective mother should be reduced to a minimum, that she may feel at liberty to lie down several times during the day on the porch or in a well-ventilated room, in the midst of the best possible surroundings. Sexual intercourse should be largely discontinued during the last months of pregnancy.
I sometimes wish the prospective mothers in our dispensary districts might have some of the care and the kind treatment which is bestowed upon an ordinary prospective mother horse, which at least enjoys a vacation from heavy labor, and whose food is eaten with calm nerves and in the quietness of a clean stall. While the state of the mother's mind does not materially influence the child; nevertheless, the state of the mother's body,54 the weary over-worked muscles and nerves of hot, tired women, bending over cook stoves, laundry tubs, or scrubbing floors, does materially derange the mother's health and digestion, which in turn, reflexly interferes with the growth and physical development of her child. Extra strength is required for the day of labor, and since the baby doubles its weight during the last two months, the mother is living for two, and should, therefore, avoid extreme fatigue, over tiring, and irksome labor during these final weeks of watchful waiting.
It may or may not be within the province of prospective parents to rearrange, rebuild, or otherwise change the home. Usually the size of the pocketbook, the bank account, or the weekly pay envelope decide such things for us. The home may be in the country or suburbs, with its wide expanse of lawns, its hedges of shrubbery, and with its spacious rooms and porches; or it may be a beautifully equipped, modern apartment on the boulevard of a city, with its sun parlors, large back porches, conveniently located near some well-kept city park, or it may be one of those smaller but "snug as a bug in a rug" apartments, in another part of the city, where usually there is a sunny back porch; or again some of my readers may themselves be, or their friends may be, in a darkened basement with broken windows, illy ventilated rooms, with no porches, no yards, no bright rays to be seen coming in through windows—and yet into all of these varied homes there come little babies—sweet, charming little babies, to be cared for, dressed, fed, and reared. And we must now proceed to the subject of making the most of what we have—to create out of what we have, as best we can, that which ought to be.
In both the country and city place, yards and alleys should be cleaned up. Garbage—the great breeding place of flies—should be removed or burned. The manure pile of the stable or alley should also be properly covered and cared for. In this way breeding places for flies are minimized and millions55 and billions of unhatched eggs are destroyed. In the large cities, provision is made for the prompt disposal of garbage, and laws are beginning to be enforced regarding the covering and the weekly removal of manure, and thus in many of our large cities flies are diminishing in numbers each year. Fly campaigns and garbage campaigns are teaching us all to realize the dangers of infection, contagion, and disease as a result of filth; while through the schools, the children of even our foreign tongued neighbors take home the spirit of "cleaning up week." Even in the rural districts we hope for the dawning of the day when filth, stagnant pools, open manure piles, and open privies, will be as much feared as scorpions or smallpox.
As suggested elsewhere, as soon as the expectant mother is aware that she is pregnant, she should engage her physician. And since these are days of specialists, he may or may not be the regular family doctor. The husband and friends may be consulted, but the final choice should be made by the prospective mother herself. "The faith which casts out fear, the indefinable sense of security which she feels in her chosen physician, supports her through the hours of confinement." Twenty-four hour specimens of urine should be saved and taken to the physician twice each month and oftener during later months of pregnancy. The chosen physician's instructions and suggestions should be carried out and counsel should be sought of him as to the place of confinement.
There are a number of factors that enter into the selection of the place of confinement. In the first place, if the home be roomy, bathroom convenient, if the required preparation of all necessities for the day of labor can be effected, and it is further possible to prepare a suitable delivery-room at home with ample facilities for emergencies and complications, and you can persuade your physician to do it—then the best place in the world for the mother to be confined is within the walls of her own home. But such is the case in but one home out56 of hundreds, and I regret that time and space will not allow me to describe and portray the many untimely deaths that might have been avoided if this or that supply had only been ready at the moment of the unexpected complication of delivery. Why should we needlessly risk the lives of prospective mothers, when, in every up-to-date hospital delivery-room, all these life-saving facilities are freely provided? Here in the modern hospital, the mothers from small homes and apartments, the mothers who live in stuffy basements, as well as those from the average home in the average neighborhood, can come with the assurance of receiving the best possible care and attention. Every woman who can arrange or afford it, should plan to avail herself of the benefits, comforts, quietness, and calm of a well-equipped hospital and the surgical cleanliness and safety of its aseptic delivery-room.
Fortunately, the mother of the basement home may have the same clean, sterile dressings used upon her as does the mother of the boulevard mansion. The maternity ward bed at $8.00 to $10.00 a week can be just as clean as the bed of the $40.00 a week room. The methods and procedures of the delivery-room can be just as good in the case of the very poor woman as in the case of the magnate's wife. In no way and for no reason fear the hospital. It is the cleanest, safest, and by far the cheapest way. The weekly amount paid includes the board of the patient, the routine care, and all appliances and supplies of every sort that will be used. Under no circumstances should a midwife be engaged. Any reputable physician or any intellectual minister will advise that. Let your choice be either the hospital or the home; but always engage a physician, never a midwife.
After selecting the place of confinement, the question of the nurse may next be considered. If it is to be the hospital, you need give little further thought to the nurse, for your physician will arrange for the nurse at the time you enter the hospital. She will be a part of the complete service you may enjoy. You will find her on duty as you, quietly resting in your room, awaken57 in the sweet satisfaction that at last it is all over—at last your baby is here.
A competent nurse is a necessity, if the confinement takes place in the home. She may be a visiting nurse, who, for a small fee, will not only come on the day of labor, but will make what is known as "post-partum calls" each day for ten or twelve days. These are short calls, but are long enough to clean up the mother and wash and dress the babe. She is not supposed to prepare any meals or care for the home. Then there is the practical nurse—women who have prepared themselves along these lines of nursing, whose fees range from $12.00 to $18.00 a week. If your physician recommends one to you, you may know she is clean and dependable. The trained nurse, who has graduated from a three years' course of training, is prepared for every emergency, and will intelligently work with the physician for the patient's welfare and comfort. Her fees range from $25.00 to $35.00 a week.
Both the practical and the trained nurses are human beings, and require rest and sleep the same as all other women do. One nurse, after having faithfully remained at her post of duty some sixty hours reminded the husband and sister of the patient that she must now have five hours of unbroken rest and they replied in a most surprised manner, "Why we are paying you $30.00 a week, and besides, we understood you were a trained nurse."
The physician usually makes arrangement with the family for competent relief for the nurse. She should have at least one to two hours of each day for an airing, and six hours out of the twenty-four for sleep.
The supplies should all be in the home and ready, as the seventh month of pregnancy draws near. In the first place, select the drawer or closet shelf where the supplies are to remain, untouched, until your physician orders them brought out. The supplies requiring special preparation and sterilization are:58
| Three pounds of absorbent cotton. | Twelve old towels or diapers. |
| One large package of sterile gauze (25 yards). | One yard of strong narrow tape for tying the cord. |
| Four rolls of cotton batting. | Three short obstetrical gowns for the patient. |
| Two yards of stout muslin for abdominal binders. | Two pairs of extra long white stockings. |
| Two old sheets. | Four T-binders. |
Other articles needed by physician, nurse, and patient are:
| Fifty bichloride of mercury tablets (plainly marked "poison"). | One good sized douche pan. |
| Four ounces of lysol. | Three agateware bowls, holding two quarts each. |
| Two ounces of powdered boric acid. | Two agateware pitchers, holding two quarts each. |
| One half ounce of 20% argyrol. | Two stiff hand-brushes. |
| One quart of grain alcohol. | One nail file. |
| One pound jar of surgeon's green soap. | One pair surgeon's rubber gloves. |
| One half pound of castile soap. | One and one-half yards rubber sheeting 36 inches wide. |
| One bottle white vaseline. | Two No. 2 rubber catheters. |
| One drinking tube. | Two dozen large safety pins. |
| One medicine glass. | Small package of tooth picks, to be used as applicators. |
| One two-quart fountain syringe. | Six breast binders (Fig. 5). |
| One covered enamel bucket or slop jar. | Six sheets. |
Just before confinement send for one ounce of fluid extract of ergot and an original pint bottle of Squibb's Chloroform.
1. The sanitary pad is used to absorb the lochia after confinement, and needs to be changed many times during the day and night; fully five or six dozen will be required. They are usually made from cotton batting and a generous layer of absorbent cotton. If made entirely from absorbent cotton they mat down into a rope-like condition. They are four and one-half to five inches wide and ten inches long. The sterile cheesecloth is cut large enough to wrap around the cotton filling and extends at both ends three inches, by which it is fastened59 to the abdominal binder. With a dozen or fifteen in each package these vulva pads are wrapped loosely in pieces of old sheets and pinned securely and marked plainly on the outside.
2. Delivery pads. These pads should be thirty-six inches square and about five inches thick, three or four inches of which may be the cotton batting and the remainder absorbent cotton. Three of these are needed. Each should be folded, wrapped in a piece of cloth and likewise marked.
3. Gauze squares. Five dozen gauze squares about four inches in size may be cut, wrapped and marked. These are needed for the nipples, baby's eyes, etc.
4. Cotton pledgets. These are cotton balls, made as you would a light biscuit with the twist of the cotton to hold it in shape. They should be about the size of the bottom of a teacup. These are thrown in a couple of pillow slips and wrapped and marked.
5. The Bobbin. Cut the bobbin or tape into four nine-inch lengths and wrap and mark.
6. The tooth picks are left in the original package and do not require sterilization.
7. Sterilization. Before steaming and baking, wrap each bundle in another wrapping of cloth and pin again securely. Mark each package plainly in large letters or initials. These packages may be sent to the hospital for sterilization in the autoclave60 or they may be steamed for one hour in the large wash boiler, by placing them loosely into a hammock-like arrangement made by suspending a firm piece of muslin from one handle of the boiler to the other. The center of the hammock should come to within five inches of the bottom of the boiler which contains three inches of boiling water. The cover of the boiler is now securely weighed down and the water boils hard for one hour, at the end of which time they are removed and placed in a warm oven to dry out. The outer wrapping may be slightly tinged with brown by this baking. After a thorough drying they are allowed to remain in the same wrappings into which they were first placed and put away in a clean drawer awaiting the "Natal Day."
Each hospital has its own methods and regulations for caring for obstetrical patients and it is well for the expectant mother to visit the obstetrical section, the delivery-room and the baby's room, that she may personally know more about the place where she is to spend from ten days to two weeks. Here she may ascertain from the superintendent just what she will need to bring for the baby. Many of the hospitals furnish all the clothes needed for the baby while in the hospital; in such instances, the hospital also launders them. Other hospitals require the baby's clothes to be brought in, in which case the mother looks after the laundry. The mother always takes her toilet articles, a warm bed jacket with long sleeves, several night dresses and a large loose kimono or wrapper to wear to the roof garden or porch in the wheel chair. Warm bedroom slippers and a scarf for the head completes the outfit.
Baby's basket on the day of confinement should contain:
| One pound of absorbent cotton. | A powder box containing powder and puff. |
| One pint of liquid albolene. | An old soft blanket in which to receive the child after birth. |
| One half ounce of argyrol (mentioned in the mother's list). | A soft hair brush. |
| Safety pins of assorted sizes. | Three old towels.61 |
| Small package of sterile gauze squares. | A pair of silk and wool stockings. |
| Scales. | A flannel skirt. |
| Diapers. | An outing flannel night dress. |
| A silk and wool shirt (size No. 2). | A woolen wrapper. |
| An abdominal band to be sewed on with needle and thread. |
By special preparation, the ordinary bedroom may be fashioned into a delivery-room. Carpets, hangings and upholstered furniture must be removed. Clean walls, clean floors, and a scrupulously clean bed must be maintained throughout the puerperium. Bathroom, and if possible, a porch should be near by. In the wealthy home, a bedroom, bathroom and the nursery adjoining is ideal; but I find that real life is always filled with anything but the ideal.
The dispensary doctor is compelled to depend upon clean newspapers to cover everything in the room he finds his patient in. The only sterile things he uses he brings with him, and should he have to spend the night, the floor is his only bed. A student who was in my service told me that there was not one article in the entire home, which consisted of but one room, that could be used for the baby. He wrapped his own coat about it and laid it carefully in a market basket and placed it on the floor at the side of the pallet on which the mother lay and by the aid of a nearby telephone secured clothes from the dispensary for the babe.
Always select the best room in the house for a home confinement. If the parlor is the one sunny room, take it; remove all draperies, carpet, etc., and make it as near surgically clean as possible. While sunshine is desirable, ample shades must be supplied, as the eyes of both mother and babe must be protected.
A three-quarter bed is more desirable than a double bed. If it is low, four-inch blocks should be placed under each leg,62 the casters having been removed to prevent slipping. The bed should be so placed that it can be reached from either side by the nurse and physician. The mattress may be reenforced by the placing of a board under it if there is a tendency to sag in the middle. Over this mattress is securely pinned the strip of rubber sheeting or table oilcloth. A clean sheet covers mattress and rubber cloth and at the spot where the hips are to lie may be placed the large sterile pad to absorb the escaping fluids. The floor about the bed is protected by newspapers or oilcloth. Good lighting should always be provided. Much trouble and possible infection may be avoided by clean bedding, plenty of clean dressings, boiled water, rubber gloves, and clean hands.
As the two hundred and seventy-three days come to a close, our expectant mother approaches the day of labor with joy and gladness. The long, long waiting days so full of varied experiences, so full of the consciousness that she, the waiting mother, is to bring into the world a being which may have so many possibilities—well, even the anticipated pangs of approaching labor are welcomed as marking the close of the long vigil. These days have brought many unpleasant symptoms, they have been days of tears and smiles, of clouds and sunshine.
The prospective mother has thought many times, "Will my baby ever come?" But nature is very faithful, prompt, and resourceful. She ushers in this harvest time under great stress and strain, for actual labor is before us—downright, hard labor—just about the hardest work that womankind ever experiences—and, as a rule, she needs but little help—good direction as to the proper method of work and the economical expenditure of energy. In the case of the average mother this is about all that is needed, and if these suggestions come from a wise and sympathetic physician—one who understands and appreciates asepsis—she may count herself as fortunately situated for the oncoming ordeal.
In the days of our grandmothers it was almost the exception rather than the rule to escape "child-bed fever," "milk leg," etc.; but in these enlightened days of asepsis, rubber gloves, and the various antiseptics, puerperal infection is the exception, while a normal puerperium is the rule; and this work of pre64vention lies in the scrupulous care taken by anyone and everyone concerned in any way with the events of the day of labor.
On this day of labor, the mother, who has gone through the long tedious days of waiting, should see to it that nothing unclean—hands, sponges, forcep, water, cloth—is allowed to touch her. Above all things do not employ a physician who has earned the reputation of being a "dirty doctor." Puerperal infection is almost wholly a preventable disease and every patient has a right to insist upon protection against it.
In a former chapter will be found a detailed description of the "delivery bed." Beside this bed, or near by, are to be found the rack on which are airing the necessary garments for the baby's reception—the receiving blanket and other requisites for the first bath—together with numerous other articles essential to safety and comfort.
There should be an easy chair in the room for the mother to rest in between her walking excursions during the first stages of labor. The sterilized pads and necessary articles mentioned in an earlier chapter are, of course, close at hand.
Regular, cramp-like pains in the lower portion of the abdomen which are frequently mistaken for intestinal colic, often beginning in the lower part of the back, and extending to the front and down the thigh, are often the first symptoms of the approaching event. With each cramp or pain the abdomen gets very hard and as the pain passes away the abdomen again assumes its normal condition. These regular cramp-like pains are the result of the early dilation of the cervix—the first opening of the door to the uterine room which has housed our little citizen through the developmental stages of embryonic life—and as a result of this stretching and dilating there soon appears that special blood-tinged mucus flow commonly known as "the show."
At this time a very thorough-going colonic flushing should be administered. The patient takes the "knee-chest" position,65 or the "lying-down" position, and there should flow into the lower bowel three pints of soapy water; this should be retained for a few moments; and after its expulsion, a short, plain water injection should be given. Now follows the preliminary general bath.
Just prior to the bath, the pubic hair should be clipped closely, or better shaved. Then should follow a thorough soap wash, with patient standing up in the tub, using plenty of soap, applied with a shampoo brush or rough turkish mit. The rinsing now takes place by either a shower or pail pour. Do not sit down in the tub. This is a rule that must not be broken, because of the danger of infection in those cases where the bag of waters may have broken early in the labor.
A weak antiseptic solution, prepared by putting two small antiseptic tablets into one pint and a half of warm water, is now applied to the body from the breasts to the knee. Put on a freshly laundered gown, clean stockings and wrapper. The head should be cleansed and hair braided in two braids.
If all the mothers who read this volume could bear children with the comfort Mrs. C. does, I should be happy, indeed.
At four o'clock one morning a very much excited father telephoned me, "Hurry, quick, Doctor, it's almost here." It was well that we did hurry, for the first sign the little mother had was the deluge of the waters—at this point the husband ran to telephone for the doctor—no more pains for thirty-eight minutes (just as we entered the door) and the baby was there. But such is not usually the case, nor will it be, as labor usually progresses along the lines of conscious dilating pains, occurring at intervals twenty minutes apart at first, later drawing nearer together until they are three to five minutes apart. This "first stage of labor" lasts from one to fifteen hours—during which time the tiny door to the uterine room which was originally about one-eighth of an inch open—dilates sufficiently to allow the passage of the head, shoulders and body of the fully developed child.
About this time the bag of waters usually bursts, and, as a66 rule, this marks the beginning of the "second stage of labor." The amount of water passed varies in amount. Should the rupture take place before the door is fully open, then labor proceeds with difficulty and the condition is known as "dry labor."
The head after proper rotation now begins the descent; and here the pains begin to change from the sharp, lancinating, cramp-like pains which begin in the back and move around to the front, to those of the "bearing down" variety, while at the same time there begins to appear the bulging at the perineum, which means that the head is about to be born. At this time great stress is brought to bear upon the perineum and often, in spite of anything that can be done to prevent it, the perineum is more or less lacerated.
As soon as the baby is born the "second stage of labor" has passed and within thirty to fifty minutes the close of the third stage of labor is marked by the passage of the placenta or "afterbirth."
Sometimes, as long as two weeks before the birth of the child, certain irregular, heavy, cramp-like pains occur in the abdomen and back. For a half-dozen pains they may show some signs of regularity; but they usually die down only to start up again at irregular intervals. These are known as "false pains."
When the pains begin to take on regularity and gradually grow heavier and it is near the appointed time for the labor, the patient should prepare to start for the hospital; or, if it is to be a home delivery, the physician should be called. As noted above, the first subjective symptom may be the rupture of the bag of waters, and it is imperative to prepare at once for the labor. It is far better to spend the day at the hospital, or even two days waiting, rather than to run the risk of giving birth to the child in a taxicab or street car; or, in the event of a home labor, to have the child born before the doctor arrives.67
It is often the case that when we need our physician the most, he is busy with another patient and cannot come, or perhaps an automobile accident detains the man of the hour. The hospital delivery always possesses this advantage over the home—physicians are always on hand. We deem it wise to relate in detail the method of procedure during the rapid birth of a child; that the husband or nurse may give intelligent and clean service.
After the patient has been given the enema and has been shaved and the bath has been administered as previously directed, the helper most vigorously "scrubs up." There are three distinct phases to the "scrubbing up": First, the three-minute scrubbing of the hands and forearms with a clean brush and green soap; to be followed by, second, the trimming and cleaning of the finger nails, for it is here, under the nails, that the micro-organism lives and thrives that causes child-bed fever or septicemia; and, third, the final five-minute scrubbing of the fingers, hands, and forearms. An ordinary towel is not used to dry the well-cleansed hands, but they are now dipped in alcohol and allowed to dry in the air.
And now if the pains are returning every three to five minutes or if the bag of waters has broken, the patient should go to bed. She will lie down on her back with the knees drawn up and spread apart. The patient, having had the cleansing bath, is now washed with the disinfectant bath (2 antiseptic tablets to 1½ pints of water), from the breasts to the knees. Another member of the family takes the outer wrappings off the sterilized delivery pad and the "clean" helper places the sterile delivery pad under the expectant mother, who is directed to "bear down" when her pains come. She may be supported during these pains by pulling on a sheet that has been fastened to the foot of the bed.
The clean, helper then sits by her constantly until the baby is born but under no circumstances should touch her until after the head appears. Immediately after the birth of the head, the shoulders usually follow with the next pain, which ought to68 occur within two or three minutes. Occasionally the face turns blue, in such an instance, the mother is directed to strain vigorously and presses down heavily on the abdomen with both her hands, this usually hurries matters materially, and the body of the child follows quickly. The baby should cry at once. If the child does not show signs of life, quick, brisk slapping on the back usually brings relief. During the birth of the head it is imperative that, in the event of liquid passing at the same time, no water or blood be sucked into the mouth by the baby. Great care must be exercised in this matter. Should the baby remain blue, lay it quickly upon its right side near the mother, and after the pulse of the cord has stopped beating the clean helper ties the cord twice, two inches from the child and again two inches from this tying toward the mother, and then the cord is cut between the two tyings with scissors that have been boiled twenty minutes.
Should there be more difficulty with the breathing of the new born child, if slapping it on the back brings no relief, its back (with face well protected) may be dipped first in good warm water, then cold, again in the warm, again in the cold—this seldom fails. The child should then be kept very warm, lying on its right side.
All this time, a member of the family has been firmly grasping the mother's abdomen, and within an hour the afterbirth passes out through the birth canal. If the physician has not yet arrived, all dressings, the pad, the afterbirth, must all be saved for his inspection.
The inside of the thighs and the region about the vagina is now washed with bichloride solution, the soiled delivery pad removed, a clean delivery pad is placed under her; an abdominal binder is applied and two sterile vulva pads are placed between the legs, and hot water bottles are put to her feet, as usually at this stage there is a slight tendency toward chilliness. She should now settle down for rest. Fresh air should be admitted into the room. There may be some hemorrhage, and if it is excessive, grasp the lower abdomen and begin to knead69 it until you distinctly feel a change in the uterus from the soft mass to a hard ball about the size of a large grape fruit; thus contraction has been brought about which causes the hemorrhage to decrease. If the doctor has not yet arrived put the baby to the breast, and place an ice bag for ten or fifteen minutes on the abdomen just over the uterus. Should there be lacerations, the doctor will attend to their repair when he comes. One teaspoonful of the fluid extract of ergot is usually given at this time, if possible get in touch with the physician before it is administered.
After the mother is comfortable, your attention is directed to the baby; the condition of the cord is noted; should it be bleeding, do not disturb the tying, but tie again, more tightly just below the former tying, and with the long ends of the tape, tie on a sterile gauze sponge or a piece of clean untouched medicated cotton, thus efficiently protecting the severed end of the cord. No further dressing is needed until the doctor arrives.
Grave disorders have arisen from infection through the freshly cut umbilical cord.
Should the doctor be longer delayed, one drop of twenty per cent argyrol should be dropped in each of the infant's eyes and separate pieces of cotton should be used for each eye to wipe the surplus medicine away.
This application must not be long neglected, for a very large per cent of all the blindness in this world might have been avoided had this medicine been placed in each eye soon after birth.
The warmed albolene is now swabbed over the entire body of the infant (this is done with a piece of cotton), the arm pits, the groins, behind the ears, between the thighs, the bend of the elbow, etc, must all receive the albolene swabbing. In a few minutes, this is gently rubbed off with a piece of gauze or an old soft towel, and the baby comes forth as clean and as smooth as a lily and as sweet as a rose.
The garments are now placed on the child—first the band,70 then shirt, diaper, stockings, flannel skirt, and outing flannel gown—and it is put to rest after the administration of one teaspoonful of cooled, boiled water. In six to eight hours it will be put to the breast.
In recent years much has appeared in both the popular magazines and the medical press concerning the so-called "twilight sleep" and other methods of producing "painless childbirth." Many of these popular articles in the lay press cannot be regarded in any other light than as being in bad taste and wholly unfortunate in their method and manner of presenting the subject; nevertheless, these writings have served to arouse such a general public interest in the subject of obstetric anesthetics, that we deem it advisable to devote two chapters to the brief and concise consideration of the subjects of pain and anesthetics in relation to the day of labor.
First, let us briefly consider the question of pain in connection with childbirth. Many women—normal, natural, and healthy women—suffer but comparatively little in giving birth to an average-sized baby during an average and uncomplicated labor. Like the Indian squaw, they suffer a minimum of pain at childbirth—at least this is largely true after the birth of the first baby; and so there is little need of discussing any sort of anesthesia for this group of fortunate women; for at most, all that would ever be employed in the nature of an anesthetic in such cases, would be a trifle of chloroform to take the edge off the suffering at the height or conclusion of labor.
But the vast majority of American mothers do not belong to this fortunate and normal class of women who suffer so little during childbirth; they rather belong to that large and growing class of women who have dressed wrong; who have lived unhealthful and sometimes indolent lives; who are more or less72 physically and temperamentally unfitted to pass through the experiences of pregnancy and the trials of labor.
The average American woman shrinks from the thought and prospect of suffering pain; she is quite intolerant with the idea of undergoing even the few brief moments of physical suffering attendant upon childbirth. She refuses to contemplate the day of labor in any other light than that which insures her against all possible pain and other physical suffering.
And it is just this unnatural and abnormal fear of labor-pains—this unwomanly dread of the slightest degree of physical suffering—that has indirectly led up to so much discussion regarding the employment of "twilight sleep" and other forms of obstetric anesthesia.
While the authors recognize the great blessing of anesthesia to the woman in labor—and almost unfailingly make use of it in some form—nevertheless, we also recognize that it would be a fine form of mental discipline and mighty good moral gymnastics, if a great many self-centered and pampered women would "spunk right up" and face the ordeal of labor with natural courage and normal fortitude. It would be "the making of them," it would make new women out of them, it would start them out on the road to real living. At the same time we do not mean to advocate that women should suffer unnecessary pain in childbirth any more than we allow them to suffer in connection with surgery.
While so much is being written about "twilight sleep" and "painless labor," it might be well to remind the American mother that much can be done to lessen the sufferings of the day of labor by one's method of living prior to the confinement.
We believe that child-bearing is a perfectly normal physical function for a healthy and normal woman—that it is even essential to her complete physical health, mental happiness, and moral well-being. Theoretically, child-bearing ought to be but little more painful than the functionating of numerous other vital organs—stomach, heart, bladder, bowels, etc.—and, in73deed, it is not in the case of certain savage tribes and other aboriginal people, such as our own North American Indian.
But we must face the facts. The average American woman does suffer at childbirth; and she suffers more than we are disposed to allow her, or more than she, as a general rule, is willing to suffer. So, while we discuss appropriate methods of lessening the pain of labor and the pangs of childbirth by the scientific use of anesthetics, let us also call attention to certain things which may aid in decreasing the amount of pain which may reasonably be expected to attend child bearing.
To assist in bringing about this preparation for decreased pain at childbirth, mothers should teach their daughters how to develop, strengthen, and preserve their physical, mental, and moral resistance. The young mother should be taught by both her mother and her physician how to dress, how to work, and how to eat. Every care should be given to the hygiene of pregnancy and labor.
The expectant mother should have plenty of fruits and fruit juices, and if not physically well endowed to give birth to a large babe, she should have her diet restricted in meat, bread and milk, as well as the cereals. Overeating during pregnancy should be carefully guarded against, as emphasized in an earlier chapter. Deformities of the pelvis, etc., should rule out a consideration of pregnancy.
While artificial painless childbirth by means of "twilight sleep" and other similar methods all have their place; nevertheless, these procedures should not lead to the neglect of those natural methods and preventive practices which aid in preparing the normal expectant mother for nature's relatively painless labor. When so much anesthesia has to be used in a normal labor, it cannot but strongly suggest that both patient and physician have neglected those common but efficient methods which contribute indirectly to lessening the pangs of child bearing.
"Twilight sleep" is a recent term which has become associated in the public mind with "painless labor." The reader74 should understand that "twilight sleep" is not a new method of obstetric anesthesia. While this method of inducing "painless labor" has been brought prominently before the public mind in recent years by much discussion and by numerous magazine articles—being often presented in such a way as sometimes to lead the uninstructed layman to infer that a new method of obstetric anesthesia had just been discovered—it has, nevertheless, been known and more or less used since 1903. Later known as the "Freiburg Method," and as the "Dammerschlaf" of Gauss, and still later popularized as "twilight sleep," this "scopolamin-morphin" method of obstetric anesthesia, has gained wide attention and acquired many zealous advocates.
"Twilight sleep" is, therefore, nothing new—it is simply a revival of the old combination of scopolamin and morphin anesthesia. While many different methods of administering "twilight sleep" have been devised, the following general plan will serve to inform the reader sufficiently regarding the technic of this much-talked-of procedure.
The scopolamin must always be fresh, although different forms of the drug are used. It tends quickly to decompose—forming a toxic by-product—and, according to some authorities, this decomposed scopolamin is responsible for many undesirable results which have attended some cases of "twilight sleep." Various forms of morphin are also used, as also is narcophin.
The "twilight-sleep" injections are not started until the patient is in the stage of active labor. The initial injection consists of the proper dose of scopolamin and morphin (or some of their derivatives), while the patient's pupils, pulse, and respiration are carefully noted, as also are the character of the uterine contractions and the character of the fetal heart action.
Usually within an hour, a second dose of scopolamin is given, while the application of so-called "memory tests" serves to indicate whether it is advisable to administer additional injec75tions. Some leading advocates of this method claim that the majority of the unfavorable results attendant upon "twilight sleep" are the direct result of failure to control the dosage of the drug by these "memory tests;" and they call attention to the large percentage of "painlessness" as proof of probable overdosing. If the patient's memory is clear and she is not yet under the influence of the drug, a third dose is soon given. If, however, the patient is in a state of amnesia (lack of memory), this third injection is not commonly given until about one hour after the second injection. The amount of amnesia present is used as a guide for repeated injections at intervals of one to one and a half hours. As a rule, the morphin is not repeated.
It must be evident that the success of such a method of anesthesia must depend entirely upon thoroughgoing personal supervision of the individual patient by a properly trained and experienced physician; and it is for just these reasons that "twilight sleep" is destined to remain largely a hospital procedure for a long time to come.
Experience has shown that those cases of "twilight sleep" that are not under the influence of scopolamin over five or six hours do vastly better than those under a longer time. When employed too long before labor this method seems to favor inertia and thus tends to increase the number of forceps deliveries.
The number of injections may run from one to a dozen or more, and patients have come through without accident with fifteen or more doses, running over a period of twenty-four hours.
While "twilight sleep" as a method of anesthesia is not altogether new, many of the claims made for it by recent advocates are more or less new; and, to enable the reader clearly to comprehend both the advantages and disadvantages of this method, both the favorable and unfavorable facts and contentions will be summarized in this connection. The favorable claims made for "twilight sleep" are:76
1. That eighty to ninety per cent of all women who use this method can be carried through a practically painless labor.
2. That there is practically no danger to the mother (some degree of danger to the child is admitted by most of its champions) other than those commonly attendant on the older and better known methods in general use.
3. That "twilight sleep," being almost exclusively a hospital procedure, would result in more women going to the hospital for their confinement—if it were used more; and would, therefore, tend to bring about more careful supervision and individual care on the part of the attending obstetrician.
4. That by lessening the dread of labor and the fear of painful childbirth, there will probably occur an increase in the birth rate of the so-called "higher classes of society"—the social circles which now show the lowest birth rates.
5. That it is of special value in the cases of certain neurotic women and those of low vital resistance; especially those patients suffering from certain forms of heart, respiratory, kidney, and other organic diseases.
6. Some authorities maintain that "twilight sleep" is of value even in threatened eclampsia, although they admit it tends to produce a rise in blood-pressure.
7. It is supposed to shorten the first stage of labor—by facilitating the dilation of the cervix—owing to the painless stretching; although the majority of its special advocates admit that it lengthens the second stage of labor, during which the patient must be very closely watched.
8. That even in those cases where the sense of pain is not entirely destroyed, the patient seems to possess little or no subsequent memory of any physical suffering or other disagreeable sensations.
9. That the method is of special value in sensitive, high-strung, nervous women of the "higher classes," who so habitually shun the rigors of child bearing—especially in the instance of their first child.
10. That the action of scopolamin is chiefly upon the central nervous system—the cerebrum—that it diminishes the perception of pain without apparently decreasing the contractile77 power of the uterus; labor may, therefore, proceed with little or no interruption, while the patient is quite oblivious to the accompanying pains.
11. That the physical and nervous exhaustion is quite entirely eliminated—especially in the case of the first labor—that patients who have had this method of anesthesia appear refreshed and quite themselves even the first day after labor.
12. That there is decidedly less "trauma" (appreciable injury) to the nervous system and therefore less "shock;" and that all this saving of nervous strain tends greatly to hasten convalescence.
13. And, finally, that "twilight sleep" does not interfere with the carrying out of any other therapeutic measures which may be deemed necessary for a successful termination of the labor.
While we are recounting the real and supposed advantages of "twilight sleep"—especially in certain selected cases—it will be wise to pause long enough to give the same careful consideration to the known and reputed dangers and drawbacks which are thought to attend this method of anesthesia in connection with labor cases.
We desire to state that these expressions, both for and against "twilight sleep," are not merely representative of our own experience and attitude; but that they also represent, as far as we are able to judge at the time of this writing, the consensus of opinion on the part of the most reliable and experienced observers and practitioners who have used and studied this method in both this country and Europe. The dangers and difficulties of "twilight sleep" may be summarized as follows:
1. That this method tends to weaken the mental resistance of many women; to lessen their natural courage and to decrease that commendable fortitude which is such a valuable feature of the character endowment of the normal woman.
2. That "twilight sleep" is essentially a hospital method and is, therefore, inaccessible to the vast majority of women belong78ing to the middle and lower classes of society, as well as to those women who live in rural communities.
3. That in fifteen or twenty per cent, the method fails to produce the desired results—at least, when administered in amounts which are deemed safe.
4. That this method does decrease the baby's chances of living; that the second stage of labor is definitely prolonged; that from ten to fifteen per cent of the babies are sufficiently under the influence of the anesthesia when born as to be unable to breathe or cry without artificial stimulus.
5. That it is a method requiring special training and experience; that it will be many years before the average practitioner will become proficient in its use; and that the older methods are probably far safer for the average physician.
6. That the method requires more care in its administration than can be expected outside of the hospital in order to avoid the dangers of fetal asphyxiation—which danger has led not a few obstetricians to abandon it.
7. That a satisfactory technic is almost impossible of development; that every patient must be individualized; that the chief dangers are connected with the over dosage of morphin; that the method is not adaptable to the general practice of the average doctor.
8. That by prolonging the second stage of labor and by sometimes giving too much morphin, the number of forceps deliveries is greatly increased, with their attendant and increased dangers to both mother and child.
9. That the prospects of passing through labor which may be rendered painless by artificial methods, tends to produce an attitude of carelessness and indifference towards those natural methods of living and other hygienic practices which so greatly contribute to naturally painless confinements.
10. That this method as sometimes practiced greatly increases the dangers of a general anesthetic, if such should be found necessary later on during the labor.
11. That "twilight sleep" is contra-indicated (should not be used) in the following conditions: primary inertia (abnormally delayed and slow labor); expected short labor—especially79 in women who have already borne children; when the fetal head is known to be large and the mother's pelvis small; placenta praevia (abnormal placental attachment); accidental hemorrhage; absent or doubtful fetal heart beat; when labor is already far advanced; and in threatened convulsions and eclampsia.
Having presented the evidence both for and against "twilight sleep," it may be of assistance to the lay reader to have placed before her the personal conclusions and working opinions of the authors. We, therefore, undertake to summarize our present attitude and outline our practice as follows:
1. "Twilight sleep" as a method of obstetric anesthesia in certain selected cases and in well-equipped hospitals, and in the hands of careful and experienced practitioners, has demonstrated that it is a scientific reality—and has probably come to stay—at least until better and safer methods of affecting a relatively painless confinement are discovered; although we are compelled to state that it is not the panacea the lay press has led many of our patients to believe. (That we believe a much better and safer method has been devised, the next chapter will fully disclose.)
2. We do not expect this method ever to become general in its use; we do not look for a chain of special "twilight hospitals" to stretch across the continent and then to overrun the country. We expect much of the recent forced enthusiasm to die down, while scopolamin-morphin anesthesia takes it proper place among other scientific methods of alleviating the pangs of labor.
3. We know that standard and fresh solutions—as already noted—are absolutely essential for the success of this method.
4. We are certain that no routine method or technic can be developed. Each patient must be individualized. The method does not consist in injecting scopolamin every so often. The patient's mental and physical condition—as also that of the unborn child—must control the administration of "twilight sleep."80
5. The patient must be in a quiet and partially darkened room. She must not be disturbed; while the physician, or a competent trained nurse, must be in constant attendance. well-appointed hospital, there is no real reason why it cannot be fairly well carried out in a well-regulated private home, provided the necessary preparations have been made, a trained nurse is present, and provided, further, that the physician is willing to remain in the home with the patient the length of time required properly to supervise the treatment.
6. While this method of treatment is best carried out in the well-appointed hospital, there is no real reason why it cannot be fairly well carried out in a well-regulated private home, provided the necessary preparations have been made, a trained nurse is present, and provided, further, that the physician is willing to remain in the home with the patient the length of time required properly to supervise the treatment.
7. Even when the treatment is not instituted early in labor, it can, in certain selected and appropriate cases, be utilized even in the second stage of labor—thus saving these special cases much unnecessary pain; in fact, some authorities regard it as a valuable adjunct in the management of "borderland contractions" as it allows the patient a full test of labor.
8. In our opinion, this method has little effect on the first stage of labor if properly administered; but it does undoubtedly prolong and tend to complicate the second stage; in fact, we are coming to look upon "twilight sleep" as being more distinctly a first stage procedure; that it bears the same relation to the first stage of labor that chloroform bears to the second stage—relieving the pain but not stopping the progress of labor.
9. That when safe amounts of the drug are used the pain is greatly lessened in all cases—the subsequent memory of pain is absent in the majority of the patients—but the labor is not always entirely painless as is popularly supposed.
10. We do not believe that this method when properly administered increases the number of forceps deliveries—at least not in the case of high forceps operations. It undoubtedly does cover up the symptoms of a threatened rupture of the uterus, and thus increases danger from that source; nevertheless it may be safely stated that this method does not in any way greatly interfere with any other measures which might be found necessary to institute in order to bring about a successful termination of the labor.
11. The baby's heart beat must be carefully and constantly watched; sudden slowing means that the treatment must be discontinued81 and the child delivered as soon as possible; even then, difficulty may be experienced in getting the baby's breathing started after it is born. In the vast majority of cases where the baby does not cry or breathe at birth, the usual methods employed in such cases serve quickly to establish normal respiration, and the baby seems to be but little the worse for the experience.
12. While altogether too much has been claimed for "twilight sleep" at the same time many false fears have also been suggested, among which may be mentioned the fear of the mother losing her mind after the treatment; the undue fear of asphyxiation on the part of the baby; the fear of post-partum hemorrhage; and the fear that it will lessen the milk supply. We cannot deny that the child's dangers are often increased; but in other respects, this method (in properly selected cases) presents little more to worry us than the older methods of anesthesia.
13. We are inclined to the belief that this method has but little influence on the course of convalescence following labor. Certain nervous and highly excitable women certainly seem to do better, as a result of experiencing less pain and nervous shock; while other cases do not turn out so well. It certainly does not retard repair and recovery during the puerperium.
14. This method seems to have its greatest field of usefulness in those cases of highly intelligent but excessively neurotic women who have an abnormal dread of pain and child bearing; or women who have suffered unusually at the time of a previous confinement—perhaps in the case of the first baby—or from other complications; women such as these, and other special cases, are the ones to benefit most from the employment of "twilight sleep."
15. This method as has already been intimated, is most useful in the case of the first baby, or in the case of women who have established a record of tedious and painful labors. It has no place in normal and short labors; although it may be used to great advantage in certain cases during the first stage of labor—being carefully and lightly administered—while chloroform or gas is utilized at the end of the second stage just as has been our custom for a generation.82
16. As noted under the special claims made for this method, it is (as also is nitrous oxid) the ideal procedure in cases of heart, respiratory, kidney, and other organic difficulties, the details of which have already been noted, and their repetition here is not necessary.
17. It must be remembered that scopolamin and morphin are more or less uncertain in their action; scopolamin is variable in its results, often producing such marked nervous excitement in the patient as greatly to interfere with the carrying out of an aseptic technic; while morphin has been shunned by obstetricians for a whole generation, because of its well-known bad effects on the unborn child as well as its interference with muscular activity on the part of the mother.
In Germany, it is said, that a great many damage suits against prominent physicians have resulted because of the alleged ill effects which have followed the use of "twilight sleep."
18. In presenting these facts and opinions regarding "twilight sleep," the reader should bear in mind that we are not only endeavoring to state our own views and experience, but also to give the reader just as clear and fair an idea of what other and experienced physicians think of the method, both favorably and unfavorably; and we will draw these conclusions to a close by citing the opinion of one or two who have had considerable experience with the method and who, in summing up their observations, say:
The disadvantages of the method are entirely with the accoucheur and not to the mother or child. It requires his presence at the bedside from the time the treatment is undertaken until the completion of labor, not so much because of any danger, but to keep the patient evenly under anesthesia on a line midway between consciousness and unconsciousness, for if she is allowed to go above that line in several instances she will have several so-called "isles of memory," and will be able to draw a picture of her labor in her mind and thus lose the benefit of the treatment.
These methods of anesthesia are very important and have merit. They should be used when properly indicated. No one should limit himself to a routine method. Each case should be individualized83 and the form of anesthesia best suited to the case in hand should be employed. For instance, in dealing with a primipara—one who is full of fear, who cannot stand pain, who is of an hysterical nature—morphin-scopolamin anesthesia is best suited in that particular case, because these drugs have a selective action when it comes to allay fear and produce amnesia. On the other hand, in a multipara who has had three or four children, whose soft parts are relaxed and who has short labors, the anesthetic of choice would be a few whiffs of chloroform as the head passes over the perineum. It is ridiculous to try to give such women the "twilight sleep." Furthermore, take the cases you see for the first time at the end of the first stage of labor, or during the second stage; these cases are best treated with the nitrous oxid and oxygen method. You have to individualize your cases. The prospective mother now consults the obstetrician early to find out if her particular case is suitable for the "twilight sleep." She has been informed that certain examinations—urine, blood pressure, etc.—are necessary. She knows that these examinations have to be made at regular intervals. In other words, we get the patients early and we can give them good prenatal care.
This chapter has been devoted to "twilight sleep;" the following chapter will consider "nitrous oxid" and other methods of anesthesia in connection with labor, and should be read along with the foregoing discussion in order to obtain an intelligent view of the whole subject of "painless labor."
Since the public has already been told so much about obstetric anesthesia, we deem it best to go into the whole subject thoroughly, so that the expectant mothers who read this book will be able to form an intelligent opinion regarding the question, and thus be in a position to give hearty cooperation to the decision of their physician to employ, or not to employ, any special form of anesthesia or analgesia in their particular case. In order to give the reader a complete understanding of "painless labor," it will be necessary to give attention to that newer and more safe method of obstetric anesthesia called "sunrise slumber." This method of anesthesia consists in the employment of nitrous oxid or "laughing gas," and will be fully considered in this chapter.
In this connection we desire to reiterate and further emphasize some statements made in the preceding chapter concerning the unnatural fear and abnormal dread of childbirth.
We feel that it is very important in connection with this new movement in obstetrics to reduce the woman's pain and suffering to the lowest possible minimum, that the trials of labor should not be overdrawn and the pangs of confinement overestimated. We must not educate the normal woman to look upon labor as a terrible ordeal—something like a major surgical operation—which, since it cannot be escaped, must be endured with the aid of a deep anesthesia.
The facts are that a very small per cent of healthy women suffer any considerable degree of severe pain—at least not after the first child. We often observe that judicious mental85 suggestion on the part of the physician or nurse in the form of encouraging words and supporting assurances tends to exert a marked influence in controlling nervousness and subduing the sufferings of the earlier labor pains.
We must not allow the efforts of medical science to lessen the sufferings of child-bearing, to rob womankind of their natural and commendable courage, endurance, and self-reliance.
We do not mean to perpetuate the old superstition that pain and suffering are the necessary and inevitable accompaniments of child-bearing—that the pangs of labor are a divine sentence pronounced upon womankind—and that, therefore, nothing should be done to lessen the sufferings of confinement. Severe and unnatural pain is not at all necessary to childbirth, and there exists no reason under the sun why women should suffer and endure it, any more than they should suffer the horrors of a very painful surgical operation without an anesthetic. In this connection, it should be recalled that analgesic drugs have been introduced into obstetric practice only during the last fifty years, while such methods of relieving pain have been used in general surgery for a much longer period. It is now only sixty-nine years since Simpson first employed anesthetic in obstetrics, while six years afterwards Queen Victoria gave her seal of approval to the use of chloroform in labor cases.
Thirty years ago, in speaking of the expectant mothers, Lusk warned us:
As the nervous organization loses in the power of resistance as the result of higher civilization and of artificial refinement, it becomes imperatively necessary for the physician to guard her from the dangers of excessive and too prolonged suffering.
Nitrous oxid, or "laughing gas," was first used in labor cases in 1880 by a Russian physician. During the last twenty-five years it has been used off and on by numerous practitioners in connection with confinement, but not until the last few years has this method of relieving labor pain come into prominent notice.
While the "laughing gas" method of obstetric anesthesia did86 not gain notoriety and publicity from being exploited in magazines and other lay publications, it did get its initial boost in a very unique and unusual manner. A gentleman who manufactured and sold a "laughing gas" and oxygen mixing machine for the use of dentists, insisted that this method of anesthesia should be used in the case of his daughter, who was about to be confined. This patient was kept under this nitrous oxid anesthetic for six hours—came out fine—no accidents or other undesirable complications affecting either mother or child, and thus another and safe method of reducing the sufferings of childbirth has been fully demonstrated and confirmed, although it had previously been known and used in labor cases to some extent.
Starting from this particular case in 1913, many obstetricians began experimental work with "gas" in labor cases; and, at the time of this writing, it has come to occupy a permanent place in the management of labor, alongside of chloroform, ether, and "twilight sleep."
The reader should understand the difference between analgesia and anesthesia. Anesthesia refers to the condition in which the patient is more or less unconscious—wholly or partially oblivious to what is going on, and, of course, entirely insensible to all pain. Analgesia is a term applied to the loss of pain sensation. The patient may not be wholly or even partially unconscious—merely under the influence of some agent which dulls, deadens, or otherwise destroys the realization of pain. This is the condition aimed at by the proper administration of any form of "twilight sleep," whether by the scopolamin-morphin method, or by the nitrous oxid ("sunrise slumber") method.
Any method of treatment which can more or less destroy the pain of labor without in any way interfering with its progress, and which in no way complicates its course or leaves behind any bad effects on either mother or child, must certainly be hailed with joy by both the patient and the physician. While chloroform has served these purposes fairly well, there have87 been numerous drawbacks and certain dangers; and it was the knowledge of these limitations in the use of both chloroform and ether, that has led to further experimentation and the development of these newer methods of producing satisfactory analgesia—freedom from pain—without bringing about such a state of profound anesthesia as accompanies the administration of the older methods.
It should be borne in mind that in using "sunrise slumber" (nitrous oxid) for labor pains, the gas is so administered that the patient is just kept on the "borderline"—in a typical "twilight" state—and not in the condition of deep anesthesia which is developed when nitrous oxid is employed by physicians and dentists as an anesthetic for major and minor surgical operations.
Analgesia is the first stage of anesthesia—the "twilight zone" of approaching unconsciousness—in which the sense of pain is greatly dulled or entirely lost, while even that which is experienced is not remembered. It seems to the authors that "gas" is the ideal drug for producing this condition whenever it is necessary, as nitrous oxid is the most volatile of anaesthetics, acts most quickly, and its effects pass away most rapidly, while its administration is under the most perfect control—it may be administered with any desired proportion of oxygen—and may be discontinued on a moment's notice. It is practically free from danger even when continued as an analgesic for several hours. Nitrous oxid never causes any serious disturbance in the unborn child, as chloroform sometimes does when used too liberally.
It will not be necessary to compare the favorable and unfavorable claims for nitrous oxid as we did the contentions for and against "twilight sleep." Whatever service "laughing gas" or "sunrise slumber" can render the cause of obstetrics we can accept, knowing full well that, in competent hands, it can do little or no harm; and this we know from the facts herewith recited and from the further fact that we have gained a wide experience with this agent in the practice of both dentistry88 and surgery. In a general way, the influence of "sunrise slumber" on mother and child may be summarized as follows:
1. It can accomplish its purpose—can quite satisfactorily relieve the mother of severe pain—when employed as an analgesic. It is not necessary to administer the gas to the point of anesthesia except at the height of suffering at the end of the second stage of labor, when the head of the child is passing through the birth canal.
2. This method can be stopped at any moment—the patient ran be brought out from under its influence entirely and almost instantaneously. It is not like a hypodermic injection of a drug which may exert a varying and unknown influence upon the patient, and which, when once given, cannot be recalled.
3. It is a method which may be used in the patient's home just as safely as in a hospital; the only drawback being the inconvenience of transporting the gas-containing cylinders back and forth. This is even now partially overcome by the improved combination gas and oxygen form of apparatus which has been devised.
4. The administration of nitrous oxid analgesia or anesthesia does not interfere with or lessen the uterine contractions or expulsive efforts on the part of the mother—at least not to any appreciable extent.
5. Just as soon as a severe uterine contraction—attended by its severe pain—begins to subside, the gas inhaler is immediately removed, and in a few seconds the patient is again conscious. It is not necessary to keep the patient continuously under the influence of the drug, as in the case of the scopolamin-morphin method of "twilight sleep."
6. This method ("sunrise slumber") is certainly far more safe in ordinary and unskilled hands than the "twilight sleep" procedure. The patient is more safe with this method in the hands of the average doctor or trained nurse.
7. It has been our experience that nitrous oxid in the smaller, interrupted and analgesic doses, actually tends to stimulate the uterine pains and contractions, while at the same time rendering the patient quite oblivious to their presence. When properly administered, the freedom from pain is perfect.89
8. Under the influence of "gas," patients often appear to "bear down" with increased energy. It certainly does not lessen their cooperation in this respect.
9. We have not observed, nor have we learned of, any cases of inertia (weak and delayed contractions), post partum hemorrhage, or shock, as a result of "laughing gas" or "sunrise slumber" analgesia.
10. This method lends itself to perfect control—it may be decreased, increased, or discontinued, at will; it may be given light now and heavy at another time; while, at the height of labor, it may be pushed to the point of complete anesthesia, if desired.
11. We have found "sunrise slumber" (nitrous oxid) analgesia to be the ideal obstetric anaesthetic, and have adopted it quite to the exclusion of both chloroform and "twilight sleep." We find that this form of analgesia has all the advantages of "twilight sleep" without any of its dangers or disadvantages.
12. A possible objection to the nitrous-oxid method is the cost, especially in the private home. The average cost in the hospitals where we are using this method runs about $2.00 for the first hour and $1.50 for each hour thereafter. This is the cost when using large tanks of gas, and is, of course, somewhat increased when the smaller tanks are used in the patient's home.
Since it was thought best to give the reader some idea of the technic for the administration of "twilight sleep," it may not be amiss to explain how "sunrise slumber" is usually employed in labor cases. The technic is very simple. The administration of the gas is generally begun about the time the patient begins seriously to complain of the severity of the second stage pains; although, of course, the gas can be given during the first stage pains if desired. In the vast majority of cases, however, we think it is best to encourage the patient to endure these earlier and lighter pains without resorting to analgesic procedures.
The form of apparatus used is the same as that employed by dentists and contains both nitrous oxid and oxygen cylinders.90 A small nasal inhaler is best, although the ordinary mouthpiece will do very well. The gasbag attached to the tank should be kept under low pressure and, as a pain begins, the patient is told to breathe quietly, keeping the mouth closed. As a rule this sort of light inhalation serves to produce the desired analgesic effect. It is not necessary to put the patient deeply under in order to relieve the pain.
It is our custom to begin "sunrise slumber" as soon as the uterine contractions become painful. The earlier the gas is started, the more oxygen should be used. Two or three inhalations will suffice to take the "edge" off the earlier and lighter pains. When the pains grow heavier we use less oxygen and permit three or four deep inhalations just before a bearing-down pain. At the first suggestion of a contraction, the patient must begin to inhale the gas; while after the patient has pulled hard on the traction strops—just as the contraction pain is passing—she is given an inhalation containing a larger percentage of oxygen.
At the beginning of a pain, pure nitrous oxid is administered, and the patient is instructed to breathe deeply and rapidly through the nose. The gasbags should be about half filled. The mixture of gas and oxygen must be determined by the severity of the pains and individual behavior of the patient.
Four to six inhalations of the gas are sufficient to produce the required analgesia in the average case. Following the first few deep inspirations through the nose, the patient can be instructed to breathe through the mouth, while the gas is well diluted with oxygen and continued until the end of the pain. In this way a satisfactory analgesia is maintained throughout the "pain" with a minimum of "gas." The proportion of oxygen used will run from nothing up to ten per cent. This procedure is repeated with the occurrence of each pain.
The use of the "mask" is just as effective as a nasal inhaler, but wastes more gas and so is more costly.
When the head is passing the perineum the gas should be pushed to the point of anesthesia, while the patient's color will suggest the amount of oxygen to be used as well as serve to control the administration of the nitrous oxid.91
For many years chloroform and ether have been used to alleviate the pains of women in labor. Valuable as these agents are when deep anesthesia is required for the carrying out of operative procedures, they have not proved satisfactory as analgesic agents. If administered in small quantities at the commencement of a strong uterine contraction, the patient does not usually inhale sufficient to abolish pain. She is then apt to be irritated and is certain to insist on being given a larger quantity. If a sufficient amount be administered to satisfy the woman, the continued repetition gradually inhibits the power both of the uterus and of the accessory muscles, so that labor is unnecessarily prolonged, and, possibly, the life of the fetus endangered. Physicians have, therefore, been accustomed to employ these drugs very sparingly, restricting their use to the very end of the second stage, during the painful passage of the head through the vulva. The results of the administration at this time are also uncertain. If delivery be rapid the woman may not be able to inhale sufficient to abolish her consciousness of pain. If it be slow she may take too much and weaken the muscular powers, thereby prolonging labor and, often, necessitating forceps delivery. It is not surprising, therefore, that the medical profession has long been hoping that a more satisfactory method of relieving the pain of labor would be found.
In summing up our conclusions regarding analgesia and anesthesia in labor cases, the authors would state their present position as follows:
1. That anesthetics or analgesics are a necessary accompaniment of confinement in this day and age; that the average labor case demands some sort of pain-relieving agent at some time during its progress; but that intelligent efforts should be put forth to limit and otherwise control their use. While we recognize the necessity for avoiding needless suffering, at the same time we must also avoid turning our women into spineless weaklings and timid babies.92
2. That we should seek to develop, strengthen, and train our girls for a normal and natural maternity; that we should study to attain something of the naturalness and the painlessness of the labors of Indian tribes; and, even if we partially fail in this effort, we shall at least leave our women with ennobled characters and strengthened wills.
3. That the scopolamin-morphin method of inducing "twilight sleep" has its place—in the hands of experts—and in the hospital; and that in many cases it probably represents the best method of obstetric anesthesia which can be employed.
4. That as a general rule and in general practice, the safest and best method of inducing the "twilight" state of freedom from severe pain, is by the use of nitrous oxid or "laughing gas"—the "sunrise slumber" method. It has been our practice to start all general ether anesthetics with "gas" for a number of years, while we have been doing an increasing number of both minor and major operations with "gas" alone.
5. That we still employ general ether or chloroform anesthesia in Cesarean sections and other major obstetric operations, although several operators are beginning to use "gas" in even these heavy cases.
6. That the intelligent and careful use of pituitary extract in certain cases of labor serves greatly to shorten the second stage; that it is of great value in certain "slow cases," and serves greatly to reduce the use of low forceps.
We have treated the subject of obstetric anesthesia in this full manner, because of the fact that so much has appeared in the public press on these subjects, and, further, because we desired that our readers should have placed before them the facts on all sides of the question just as fully as a work of this scope would permit.
Popularly spoken of as the "lying-in period," and medically known as the puerperium, this time of convalescence immediately following childbirth is usually occupied by two important things: the restoration of the pelvic organs to their normal condition before pregnancy, and the starting of that wonderfully adaptative mechanism concerned with the production of the varying and daily changing food supply of the offspring.
The uterus, now more than fifteen times its normal size and weight, begins gradually to contract and assume its normal weight of about two ounces; and it requires anywhere from four to eight weeks to accomplish this involution. In view of all this it is obvious that there can be no fixed time to "get up." It may be at the end of two weeks, or it may not be until the close of four or five weeks, in the case of the mother who cannot nurse her child; for the nursing of the breast greatly facilitates the shrinking of the uterus. Extensive lacerations may hinder the involution as well as other accidents of childbirth, so it must be left with the physician to decide in each individual case when the mother may enter into the activities of life and assume the responsibilities of the care of the baby and the management of her home.
During this period of the puerperium a member of the family, a neighbor, a visiting nurse, a practical nurse, or a trained nurse, looks after the mother and gives to the babe its first care; whoever it may be, certain laws of cleanliness must be carried out if infection is to be guarded against. If there are94 daily or semi-daily calls made by the physician, a member of the family may be trained to care for the mother with proper cleanliness and asepsis; but it is far better for the mother, if possible, to secure the services of a trained nurse, or the visiting nurse, in which instance she will call each day, wash and dress the baby, clean up the mother and care for the breasts. She is not supposed to clean the room, make the bed or prepare the food. If a trained nurse can be in charge, the convalescing time is usually shortened as the responsibilities are taken from the mother, her mind freed from care and it is her's to improve, rest, and wait for the restoration of the pelvic organs, when she may again go forth among her family.
The nurse may have to sleep in the same room; but, if it be possible, she should occupy an adjoining room, she should have a regular time each day for an hour's walk in the fresh air, she should be served regular meals, and be allowed some time out of the twenty-four hours for unbroken slumber. In return she will intelligently cooperate with the physician in bringing about the restoration of body and upbuilding of the mother's nerves.
From a monetary standpoint there can be nothing so wasteful or extravagantly expensive in the home as to allow the mother to drag about from day to day and week to week with chronic weakness or invalidism because she did not have proper care during her already too short puerperium, or because she got up too soon.
Having a baby is a perfectly normal, physiological procedure. It is also, usually, downright hard work; and, beside the hard laborious work, there is not only a wearied and severely shocked nervous system to be restored, but there is also a certain amount of uterine shrinkage which must take place—and this requires from four to eight weeks; and so our mother must be allowed weeks or even a month or two to rest, to enjoy a certain amount of well-directed exercise, to have an abundance of fresh air, to be wheeled or lifted out of doors if possible into the sunshine, that she may be the better prepared for the additional duties and responsibilities the little new comer entails. Sunshine and95 fresh air are wonderful health restorers as is also a well-directed cold water friction bath administered near the close of the second week of a normal puerperium. During the second week a few carefully selected exercises such as the following are not only beneficial, but tend to increase circulation and thus to promote the secretion of milk and the shrinking of the uterus.
A splendid tonic circulatory bath may be administered at the close of the second week (in normal puerperium), known as the "cold mitten friction," which is administered as follows: The patient is wrapped in a warm blanket, hot water bottle at feet, and each part of the body—first one arm then the other; the chest, the legs, one at a time—is briskly rubbed with a coarse mit dipped in ice water. As one part is dried it is warmly covered, while the next part is taken, and so on until the entire body has been treated. The body is now all aglow, the blood tingling through the veins, and the patient refreshed by this wide-a-wake bath. Properly given, the cold-mitten friction bath is one of the most enjoyable treatments known and under ordinary conditions, if intelligently administered, may be given as early as the eighth day.
After the birth of the first baby the uterus usually is in a state of constant contraction, hence there are no "after pains;" but after the birth of the second or third child, the uterine muscle has lost some of the tone of earlier days—there is a tendency toward relaxation—so that when the uterine muscle does make renewed efforts at contraction, these "after pains" are produced. They usually disappear by the third day. Nothing should be done for them, indeed they should be welcomed, for their presence means good involution (contraction) of the uterus.96
Careful notations of the temperature should be made during the first week. A temperature chart should be accurately kept and if the temperature should rise above 100° the physician should be notified at once. The third day temperature is watched with expectancy, for if an accidental infection occurred at the time of labor, it is usually announced by a chill and sudden rise of temperature on the third day. This may be as good a place as any to mention the commonly met night sweating. This is due to a marked accentuation of the function of the skin. It is not at all unusual for a sleeping mother in the early puerperium to wake up in a sweat with night gown very nearly drenched. The gown should be changed underneath the bedding, while alcohol is rubbed over the moistened skin surface.
These sweats will disappear as soon as the mother begins to regain her strength. A vinegar rub administered on going to bed may often prevent these sweats.
Immediately after the birth of the baby and the expulsion of the afterbirth, the thighs and vulva are cleansed as follows: Into a basin of warm, boiled water are dropped four small antiseptic tablets of bichlorid of mercury; this gives a proper antiseptic wash. Into this solution are placed four pieces of sterile cotton Two of these are used, one at a time, without being returned to the solution to wash each inside of the thigh, the remaining two to cleanse the vulva. Without drying the vulva, two sterile pads are applied and pinned to the binder. These pads are changed every hour during the first day or two because of the profuse lochial flow.
After each urination and bowel movement, a lysol solution (prepared by putting one teaspoonful of lysol in a quart of sterile water) is poured from a clean pitcher over the vulva into the bed pan, and fresh pads applied. This toilet continues until the close of the second week or longer, if there is a lochial flow.97
These sterile pads not only absorb the lochia but also, among ignorant or thoughtless mothers, prevent contamination by the patient's hands.
The patient should be encouraged to urinate during the first few hours after labor; catheterization should not take place until every effort has been made to bring about normal urination; or, until there is a well marked tumor above the bony arch of the pelvis in the lower part of the abdomen. It is far less harmful to the patient for her to sit up on the jar placed on the edge of the bed, than to undergo the risk of inflammation of the bladder which so often follows catheterization.
The first few days the lochia is very red because of the large amount of blood which it contains. After the third or fourth day it is paler and after the tenth it assumes a whitish or yellowish color. During the three changes it should always smell like fresh blood. Any foul, putrifying odor should be promptly reported to the physician.
If on getting up at the close of the second week the lochia should resume its red color, the patient should return to bed and notify her physician.
After the tenth day, the abdominal binder may be pinned as tightly as the patient desires, but prior to the tenth day many physicians believe the exceedingly tight binder causes misplacements of the enlarged, softened, and boggy uterus. It should be pinned snugly; but not drawn as tight as possible with the idea of keeping the uterus from relaxing, for at best, it does not do it; while tight constriction may produce a serious turning or flexion of the uterus. The breast binder is applied during the first twenty-four hours to support the filling breasts, loosely at first, and as they increase in size, as the glands become engorged, the binder is drawn more tightly. A sterile piece of gauze is placed over the nipples.98
On the morning of the second day a cathartic is usually given—say one ounce of castor oil or one-half bottle of citrate of magnesia. The bowels should move at least once during each twenty-four hours; if they are obstinate, a simple laxative may be nightly administered. Certain constipation biscuits, sterilized dry bran, or agar-agar may be eaten with the breakfast cereal. Prunes and figs should be used abundantly. Bran bread should be substituted for white bread. The enema habit is a bad one and should not be encouraged; however, the enema is probably less harmful than the laxative-drug habit. Mineral oil is useful as a mild laxative, and does not produce any bad after results.
Fissures of the nipples should be reported to the physician at once. There are many good remedies which the physician may suggest; in his absence, Balsam Peru may be advantageously applied. Boracic acid solution should be applied before and after each nursing from the very first day; in this way much nipple trouble may be prevented through cleanliness and care. The nipples should be kept thoroughly dry between nursings Nipple shields should be used where fissures persist.
For the first three days a liquid and soft diet is followed such as hot or cold milk, gruels, soups, thin cereals, eggnog (without whiskey), eggs, cocoa, dry toast, dipped toast, or cream toast. There should be three meals with a glass of hot milk at five in the morning (if awake) and late at night; nothing between meals except plenty of good cold water. After the third day, if temperature is normal, a semi-solid diet may be taken, such as baked, mashed, or creamed potatoes, soups thickened with rice, barley or flour, vegetables (peas, corn, asparagus, celery, spinach, etc.); eggs, light meats, stale breads, toast, bland or subacid fruits (sweet apples, prunes, figs, dates, pears, etc.); macaroni, browned rice (parched before steaming), etc.; ice cream, custards, and rice puddings for desserts after99 the seventh day. Three good meals a day, at eight and one and six, with a couple of glasses of hot milk or cocoa or an eggnog at five a. m., to be repeated at 9 or 10 p. m., with plenty of cold water between the meals, will abundantly supply the necessary milk for the growing babe. Tea and coffee are not of any special value in encouraging a flow of milk.
The constant coaxing of the mother with "Do drink this," and "You must drink this, or you won't have any milk," not only saddens her but seriously upsets digestion and thus indirectly interferes with normal lactation.
Everybody should stay at home and away from the mother and her new born child until after the seventh day, and then, if our patient is normal, visitors may call, but should not stay longer than five minutes. The convalescing mother will improve faster without the neighborhood gossip, or the tales of woe so often carried by well-meaning, but woefully ignorant acquaintances.
When the hard ball-like mass can no longer be felt in the lower abdomen, when the lochia has passed through the three changes already mentioned, and the flow is whitish or yellowish, scanty and odorless, the patient may sit up in a chair increasingly each day. Such conditions are usually found anywhere from the tenth to the fifteenth day. The patient first sits up a little in a chair—she has already been exercising some in bed—and this enables her to sit up with ease for a half-hour the first day, increasing one-half hour each day during the week following. At the end of three weeks, she may be taken down stairs providing there is ample help to carry her back up stairs. After another week (at the close of the fourth), if the lochia is entirely white or yellow, with no blood, she may begin carefully to go about the house. There should be no lifting, shoving, pulling, wringing, sweeping, washing, ironing, or other heavy exercise for at least another two weeks, better four weeks. Any variance from this program usually means backache, lassitude, diminished milk supply, and frequently a general invalidism for weeks or months—sometimes years.100
Cystitis, or painful urination, is avoided by tardy "getting up;" quietly, slowly moving about; abundant water drinking; and the avoidance of catheterization.
Hemorrhage. Notify the physician if it occurs at any time. The treatment is heavy kneading of the abdomen until the uterus again becomes like a hard ball. Cold compresses over the lower abdomen may sometimes help.
Infection is manifested by chilly sensations or a distinct chill followed by fever, usually on the third day. Take a cathartic; notify the physician at once and follow his directions.
Mastitis, inflammation or caking of the breasts. Very hot fomentations wrung out of boiling water, alternating with ice-cold compress, should be applied to the breast for an hour or more, three or four times a day. Cathartics should be administered, and eliminative measures instituted such as the hot-blanket pack.
Pneumonia. Keeping the arms and chest well protected by a long-sleeved coat of warm texture, should help in preventing this serious complication. Pneumonia complicating labor is usually the result of carelessness and exposure.101
Happy is the mother and fortunate is the home that possesses the intelligent services of a trained attendant during the early days of the baby's career. A century or more ago skilled nurses were unheard of, and both mothers and babies seemed to thrive on the unskilled but faithful and sympathetic care given by the willing neighbor who "thought I'd just run over and help out." Who of us cannot remember the days when mother was "gone to a neighbor's" to give this same willing but unskilled care at the time of "confinement."
And why are we so concerned today about asepsis, sterilization, etc., when a generation ago they were not? We used to live more slowly than we do now. Then it took the entire day to do the marketing for the week, now we take a receiver from the hook and a telephone wire transmits the verbal message. Our days are literally congested with events that were almost impossibilities a century ago. The ease and leisure of former days are unknown and unheard of today. The artificial way in which we live exerts more or less of a strain upon the present generation; the average woman's nervous system is keyed up to a high pitch; her general vital resistance is running at a low ebb; while child-bearing brings a certain added stress and strain that requires much planning to avoid and overcome.
For many days and ofttimes weeks the mother is unfit—physically unable—properly to care for her child, and so104 whether it be the trained assistant in constant attendance or the visiting nurse in her daily calls, or the kind, willing, but unskilled neighbor—each helper must acquaint herself, in varying degrees, with the physical, nervous, and mental needs of the child, as well as take into account and anticipate the numerous habits and wants of the new born babe, such as urination, bowel movement, pulse, respiration, temperature, etc.
At birth, the head is remarkably large as compared to the rest of the body, for, surprising as it may seem, the distance from the crown to the chin is equal to the length of the baby's trunk; and, too, if birth has been prolonged this large head has also been pressed or squeezed somewhat out of shape. This state of affairs, however, need give no cause for either alarm or anxiety, for the head will shape itself to the beautiful rotundity of the normal baby's head within a few days.
The general shape of the baby's head, as seen from above is oval. Just back of the forehead is formed a diamond-shaped soft spot known as the anterior fontanelle which should measure a little more than one inch from side to side. On a line just posterior to this soft spot and to the back of the head, is found another soft spot somewhat smaller than the one in front. Gradual closure of these openings in the bones occurs, until at the end of six or eight months, the posterior fontanelle is entirely closed; while eighteen months are required for the closure of the anterior fontanelle.
These "soft spots" should not be depressed neither should they bulge. The head is usually covered with a growth of soft, silky hair which will soon drop out, to be replaced, however, by a crop of coarser hair in due season. The scalp should always be perfectly smooth. Any rash or crusts or accumulation of any kind on the scalp is due to uncleanliness and neglect, and should be carefully removed by the thorough application of vaseline followed by a soap wash. The vaseline should be applied daily until all signs of the accumulation are entirely removed. The eyes of all babies are generally varying tints of blue, but usually change to a lighter or darker hue by the105 seventh or eighth week. The whitish fur which often is seen on the baby's tongue is the result of a dry condition of the mouth which disappears as soon as the saliva becomes more abundant.
The baby's chest, as compared to the size of the head and abdomen, appears at a disadvantage, while the arms are comparatively short and the legs particularly so, since they measure about the same as the length of the trunk. They naturally "bow in" at birth so that the soles of the feet turn decidedly toward each other. All these apparent deformities, as a rule, right themselves without any help or attention whatsoever.
The pulse may be watched at the anterior fontanelle or soft spot on top of the head while the child quietly sleeps and should record, at varying ages, as follows:
| At birth | 130 to 150 |
| First month | 120 to 140 |
| One to six months | about 130 |
| Six months to one year | about 120 |
| One to two years | 110 to 120 |
| Two to four years | 90 to 110 |
The above table is correct for the inactive normal child. Muscular activity, such as crying and sucking, increases the pulse rate from 10 to 20 beats per minute.
The respiration of the baby often gives us no small amount of real concern at the first. The baby may be limp and breathless for some few moments at birth, and this condition calls for quick action on the part of the nurse and doctor.
The utmost care to avoid the "sucking in" of any liquid or blood during its birth must be exercised, for this often seriously interferes with the breathing. Sometimes this condition is not relieved until a soft rubber catheter is placed in the throat and the mucus is removed by quick suction. When you are reasonably sure that there is no more mucus in the throat,106 then sudden blowing into the baby's lungs (its lips closely in touch with the lips of the nurse or physician) often starts respiration. Slapping it on the back also helps, while the quick dip into first hot then cold water seldom fails to give relief.
A quiet-sleeping infant breathes as shown below at varying ages. An increase of six to ten breaths per minute may be allowed for the time it is awake or otherwise active.
| At birth and for the first two or three weeks | 30 to 50 |
| During the rest of the first year | 25 to 35 |
| One to two years | about 28 |
| Two to four years | about 25 |
The normal weight of the average baby is seven to seven and one-half pounds. Its length may range anywhere from sixteen to twenty-two inches.
There is an initial loss of weight during the first few days; however, after the milk has been established the child should make a weekly gain of four to eight ounces until it is six months old, after which time the usual gain is from two to four ounces per week.
If the weight has been doubled at six months and the weight at one year is three times the birth weight, the child is said to have gained evenly and normally.
At birth the skin of the baby is red and very soft owing to the presence of a coating of fine down. A blue-tinged skin may be occasioned by unnecessary exposure or it may be due to an opening in the middle partition of the heart which should close at birth. As soon as the baby is born, it should be placed on its right side while the cord is being tied, as this position facilitates closure of this embryonic heart opening. With the provision for a little additional heat the blue color should disappear, if it is not due to this heart condition. At the close of the first week the red color of the skin changes to a yellow tint due to the presence of a small amount of bile in the blood. This sort of jaundice is very common and is in no wise evidence107 of disease. The "down" falls off with the peeling of the skin which takes place during the second week; by the end of which time, the skin is smooth and assumes that delightful "baby" character so much admired.
The cut end of the tied umbilical cord is swabbed and squeezed with a sterile sponge saturated with pure alcohol. It is then wrapped in a sterile dressing made as follows: Four or five thicknesses of sterile cheese cloth are cut into a four-inch square with a small hole cut in the center and one side cut to this center. This is slipped about the stump of the cord and wrapped around and about in such a manner as entirely to cover the stump of the cord. The wool binder is then applied and sewed on, thus avoiding both pressure and the prick of pins. If it remains dry this dressing is not disturbed until the seventh or eighth day, when the cord ordinarily drops off. Should it become moistened the dressing is removed and the second dressing is applied exactly like the first.
The closed eyes of the newly born child are generally covered with mucus which should be carefully wiped off with a piece of sterile cotton dipped in boracic acid solution, in a manner not to disturb the closed lid. A separate piece of cotton is used for each eye and the swabbing is done from the nose outward. The physician or nurse drops into each opened eye two drops of twenty per cent argyrol, the surplus medicine being carefully wiped off with a separate piece of cotton for each eye. The baby should now be placed in a darkened corner of the room, protected from the cold.
The eyes are washed daily by dropping saturated solution of boracic acid into each eye with a medicine dropper. Separate pieces of gauze or cotton are used for each eye.
As soon as the cord and the eyes have received the proper attention and the mother has been made comfortable, the baby108 is given its initial bath of oil. This oil may be lard, olive oil, sweet oil, or liquid vaseline. The oil should be warmed and the baby should be well covered with a warm blanket and placed on a table which is covered with a thick pad or pillow. The temperature of the room should be at least eighty degrees Fahrenheit. Quickly, thoroughly, and carefully the entire body is swabbed with the warmed oil—the head, neck, behind the ears, under the arms, the groin, the folds of the elbow and knee—no part of the body is left untouched, save the cord with its dressing. This oil is then all gently rubbed off with an old soft linen towel.
After the oil bath, the silk and wool shirt (size No. 2), the diaper and stockings are quickly put on to avoid the least danger of chilling. The band having been applied at the time of the dressing of the cord, our baby is now ready for the flannel skirt. This should hang from the shoulders by a yoke of material adapted to the season, cotton yoke without sleeves if a summer baby, and a woolen yoke with woolen sleeves if a winter baby. The outing-flannel night dress completes the outfit and should be the only style of dress worn for the first two weeks. Loosely wrapped in a warm shawl, the baby is about ready for its first nap, save for a drink of cooled, boiled water.
This cooled, boiled, unsweetened water should be given in increasing amounts every two hours until the child is two or three years of age. It is usually given the child in a nursing bottle. In this way it is taken comfortably, slowly, can be kept clean and warm, and should the babe be robbed of its natural food and transferred to the bottle as a substitute for mother's milk, it will already be acquainted with the bottle and thus one-half of a hard battle has already been fought and won.
The baby's bed should be separate and apart from the mother's. It may be a well-padded box, a dresser drawer, a clothes basket, or a large market basket. A folded comfortable109 slipped in a pillow slip makes a good mattress. A most ideal bed may be made out of a clothes basket; the mattress or pad should come up to within two or three inches of the top, so the baby may breathe good fresh air and not the stale air that is always found in a deeply made bed. Into this individual bed the baby is placed as soon as it is dressed; and a good sleep of four to six hours usually follows.
Frequent observations of the cord dressing should be made as occasionally hemorrhage does take place, much to the detriment of the babe. If bleeding is at any time discovered the cord is retied just below the original tying. By the time baby has finished a six- or eight-hour nap the mother is wondrously refreshed and is ready to receive it to her breast.
During the first two days the baby draws from the breasts little more than a sweetened watery fluid known as the colostrum; but its intake is essential to the child in that it acts as a good laxative which causes the emptying of the alimentary tract of the dark, tarry appearing stools known as the meconium. On the third day this form of stool disappears and there follows a soft, yellow stool two or three times a day.
The child should be put to the breast regularly every four hours; two things being thus encouraged: an abundant supply of milk on the third day and the early shrinking of the uterus. More than once a mother has missed the blessed privilege of suckling her child because some thoughtless person told her "why trouble yourself with nursing the baby every four hours, there's nothing there, wait until the third day;" and so when the third day came, there was little more than a mere suggestion of a scanty flow of milk, which steadily grew less and less.
The urine of the very young child should be clear, free from odor and should not stain the diaper, nor should it irritate the skin of the babe. Often urination does not take place for several hours, sometimes not at all during the first twenty-four hours. If the infant does not show signs of distress, there is110 no cause for alarm; the urine should pass, however, within thirty hours. As a rule there are usually between ten and twenty wet diapers during each twenty-four hours. The following table shows about the amounts of urine at different ages:
| Birth to two years | 8 to 12 ounces |
| Two to five years | 15 to 25 ounces |
| Five to ten years | 25 to 35 ounces |
The foreskin of the male child is often long, tight, and adherent, and is often the direct cause of irritability, nervousness, crying, and too frequent urination. It should be closely examined by both physician and nurse and when the foreskin does not readily slip back over the acorn-like head of the organ, circumcision is advised early in the second week. This simple operation will start the child out on his career with at least one moral handicap removed and one desirable possibility established—that of being able to keep himself clean.
The dressings that are loosely applied at the time of the operation should remain untouched (especially those next to the skin), unless otherwise directed by the physician, until the seventh or eighth day when the babe is placed in a warm soap bath, at which time the dressings all come off together. Clean sterile gauze is so placed as entirely to protect the inflamed skin from the diaper at all times before this bath, and these same dressings should be continued for at least another week. Sterile vaseline (from a tube) should be applied twice a day after the original dressings are removed in the bath at the end of the first week. There should be little or no bleeding following the operation, neither should the penis swell markedly; if either complication should occur, the physician should be promptly notified.
The girl baby is often neglected in respect to the proper care of the genitals. The lips of the vulva should be separated and 111thorough but careful cleaning should be the daily routine. The foreskin or covering of the clitoris should not be adherent; while the presence of mucus, pus, or blood in the vulva should be at once reported to the physician; in his absence, the application of twenty per cent argyrol should be made daily.
Let us thoroughly come to understand the very first day the little one's life, that it was not sent to us because the family needed something to play with; it is not a ball to toss up, neither is it a variety show. It is a tiny individual, and your responsibilities as parents and caretakers are very great. The child was sent to be fed, clothed, kept warm, dry, and otherwise cared for by you, until such a time as it will become able to care for itself. Remember, what we sow, that shall we also reap. If we sow indulgence we shall reap anger, selfishness, irritability, "unbecomingness"—the spoiled child. At two or three days the baby learns that when it opens its mouth and emits a holler, someone immediately comes. If we do it on the second and third day, why should we object to run, bow, and indulge on the one hundredth and second day?
Handle the baby as little as possible. Turn occasionally from side to side, feed it, change it, keep it warm, and let it alone; crying is absolutely essential to the development of good strong lungs. A baby should cry vigorously several times each day. If the baby is to be handled, support the back carefully (Fig. 6).
During the first week the baby is oiled daily over his entire body, with the exception that the cord dressing remains untouched. The face, hands, and buttocks are washed in warm water. After the third week the bathroom is thoroughly warmed and the small tub is filled with water at temperature of 100 F. The baby having been stripped and wrapped in a warm turkish towel, is placed on a table protected by a pillow, while the caretaker stands by and vaselines the creases of the neck, armpits, folds of the elbows, knees, thighs, wrists, and genitals; and then, with her own hands, she applies soap suds all over112 the body—every portion of which is more quickly and readily reached—than by the use of a wash cloth. And now, with the bath at 100 F., with a folded towel on the bottom of the small tub, the soapy child is placed into the water and after a thorough rinsing is lifted out again to a warm fresh towel on the table and the careful drying is quickly begun. After the bath all the folds and creases are given a light dusting with a good talcum.
During hot weather the bath should be given daily, soap being used twice a week. On the other days there should be the simple dipping of the child into the tub. During the cold weather the full bath is given but twice a week, while on the other days a sponge bath or an oil rub may be administered.
A weak, delicate child should not be exposed to the daily full bath, but rather the semi-weekly sponge bath and the daily oil rub should be administered. We have found the late afternoon hour to be better than the early morning hour for baby's bath. It requires too much vital resistance to react to an early morning bath, especially when the house is cool.
The use of soap is very much abused with young babies. I recall one mother who came into the office with her poor little baby which was constantly crying and fretting because of a greatly inflamed body—all a result of the too frequent use of soap. I said, "I am afraid you do not keep your baby clean." "O Doctor!" she replied, "I wash him with soap every time I change him; I am sure he is clean." And come to find out, the poor little fellow's tender skin had been subjected to soap several times a day. We ordered the use of all soap discontinued, vaseline and talcum powder to be used instead, and the child's skin got well in a very short time.
Tight bands should not be placed about the babe. If the umbilicus protrudes, do not endeavor to hold it in by a tight band, but consult your physician about the use of a bit of folded cotton and adhesive plaster, and then allow the child the free113dom of the knitted bands, with skirts suspended from yokes. The day of tight bands and pinning blankets with their additional and traditional windings is over. After the complete healing of the cord, the need for a snug binder to hold the dressings in place is over. Should the baby cry violently, the umbilicus should be protected in the manner described above—the fold of cotton and the adhesive plaster.
The diaper, stockings, shirt, skirt, and dress with an additional wrapper for cold days completes the outfit at this age.
"One of the most important services to render the newborn baby is to have his birth promptly and properly registered."
In most states the attending physician or midwife is required by law to report the birth to the proper authority, who will see that the child's name, the date of his birth, and other particulars are made a matter of public record. Birth registration may be of the greatest importance when the child is older, and parents should make sure this duty is not neglected.
A public health official some time ago epitomized some of the uses of birth registration as follows:
There is hardly a relation in life from the cradle to the grave in which such a record may not prove to be of the greatest value. For example, in the matter of descent; in the relations of wards and guardians; in the disabilities of minors; in the administration of estates; the settlement of insurance and pensions; the requirements of foreign countries in matters of residence, marriage, and legacies; in marriage in our own country; in voting and in jury and militia service; in the right to admission and practice in the professions and many public offices; in the enforcement of laws relating to education and to child labor, as well as to various matters in the criminal code; the irresponsibility of children under ten for crime or misdemeanor; the determination of the age of consent, etc., etc.
We wish it were possible for every mother who reads this book to have a special baby's room or nursery. Some of our readers have a separate nursery-room for the little folks, and so we will devote a portion of this chapter to the description of what seems to us a model arrangement for such a room; but, realizing that ninety-five per cent of our readers can only devote a corner of their own bedroom to the oncoming citizen, we have also carefully sought to meet their needs and help them to take what they have and make it just as near like the ideal nursery as possible.
The nursery should be a quiet room with a south or southwesterly exposure. The bathroom should adjoin or at least be near. A screened-in porch is very desirable.
Draperies that cannot be washed, and upholstered furniture, do not belong in the baby's room. A hardwood floor is better than a carpet or matting; while a few light-weight rugs, easily cleaned, are advisable. Enameled walls are easily washed and are, therefore, preferable to wall paper or other dressings.
The windows should be well screened, for by far the greatest dangers to which the baby is exposed, are flies and mosquitoes—carriers of filth and disease. Flies, mosquitoes, cockroaches, bed bugs, cats, dogs, lice, and mice are all disease carriers and must therefore be kept out of baby's room.
At each window should be found dark shades, and if curtains are desired they should be of an easily washable material, such115 as mull, swiss, lawn, voile, or scrim. The hardwood floor may be covered where necessary with easily handled rugs which should be aired daily. The other necessary articles of furniture are a crib of enameled iron whose bedding will be described elsewhere in this chapter, a chest for baby's clothes and other necessary supplies, a screen or two, a low table and a low rocker, a small clothes rack on which to air the clothes at night, a pair of scales, and a medicine chest placed high on the wall.
If the room will conveniently admit it, a couch will add greatly to the mother's comfort; and, if possible, it should be of leather upholstery; otherwise, it should possess a washable cover, for all articles that promote the accumulation of dust are not to be allowed in the nursery. In these early weeks and months baby will not benefit from pictures or other wall decorations, and so let him have clean walls that are easily washed and quickly dusted.
The necessities for baby's personal care are:
| Talcum powder. | Sterile cotton balls in covered glass jar. |
| Castile soap. | Safety pins of different sizes. |
| Soft wash cloths. | Hot water bag with flannel cover. |
| Soft linen towels. | Baby scales. |
| Bottle of plain vaseline. | Drying frames for shirt and stockings. |
| Boracic acid, oz. iv (Saturated Solution). | |
| Olive oil. |
Since the days of Solomon, accidents have occurred where mother and babe have occupied the same bed. Not only is there the ever-present danger of smothering the babe, but there are also many other reasons why a baby should have its own bed. The constant tendency to nurse it too often and the possibility of the bed clothing shutting off the fresh air supply, are in and of themselves sufficient reasons for having a separate bed for baby.
The first bed is usually a basinet—a wicker basket with high sides—with or without a hood. A suitable washable lining116 and outside drape present a neat as well as sanitary appearance. The mattress of the basinet is usually a folded clean comfort slipped into a pillow slip; this is to be preferred to a feather pillow, as it is cooler and in every way better for the babe.
Drapes about the head of the basinet are not only often in the way, shutting out air, etc., but they also gather dust and are unsanitary. Screens are movable—they may be used or put away at will—and are, therefore, very convenient about the nursery.
The basinet may be dispensed with entirely if the sides of the enameled crib are lined to cut off draughts and the babe is properly supported by pillows. After the baby is four to six months of age it is transferred to the crib. The basinet has an advantage over the crib during those early weeks in that its high sides protect the babe from draughts, and the comforts and blankets can be more easily tucked about the little fellow to keep him warm. The sides should not extend more than four inches above the lying position of the child.
The enameled iron crib should be provided with a woven-wire mattress, over which is placed a mattress; hair is best as a filling for the mattress, wool next, and cotton last. Over the mattress should be placed a rubber sheet, and over all a folded sheet.
A pillow of hair or down is not to be discarded; for recent investigation has shown that the pillow favors nasal drainage, while lying flat encourages the retaining of mucus in the nose and nasal chambers—the sinuses. The pillow slip should be of linen texture.
During the winter a folded soft blanket over the rubber sheet increases both softness and warmth. No top sheet is used during the first months, particularly if the first months are the winter months. The baby is wrapped loosely in a light weight clean blanket or shawl, and other blankets—as many as the season demands are tucked about the child. These blankets should be aired daily, and the one next to the baby changed, aired, or washed very often.117
To prevent baby from becoming uncovered the sleeping blanket has been devised. The blanket is folded and stitched in such a way as completely to envelop the sleeping babe, and at the same time afford the utmost freedom (Fig. 7). The babe may turn as often as he desires, but cannot possibly uncover himself. Bed clothes fasteners are also used—an elastic tape being securely fastened to the head posts and then by means of clamps or safety pins attachment is made to the blankets on either side. The elasticity allows considerable freedom to the child in turning (See Fig. 8).
The subject of ventilation has been so fully discussed by the authors in another work that we refer the reader to The Science of Living, or the Art of Keeping Well.
For the first two or three weeks the nursery temperature should be maintained at seventy degrees Fahrenheit by day and from sixty degrees to sixty-five degrees by night. In the third week the day temperature should be sixty-eight degrees Fahrenheit measured by a thermometer hanging three feet from the floor. After three months the night temperature may go as low as fifty-five degrees Fahrenheit, and after the first year it may go as low as forty-five degrees.
The heating of the nursery is usually controlled by the general heating plant, and no matter what system of heating is maintained, humidifiers must be used, the necessity for which is doubled when the system is that of the hot-air furnace.
These shallow pans of water with large wick evaporating surfaces will evaporate from three to four quarts during the twenty-four hours. The humidity should be fifty throughout the seasons of artificial heating.
Many colds may be entirely avoided by the use of humidifiers or evaporators. The open grate is one of the very best means of nursery heating. Gas and oil heaters should not be depended upon for nursery heat. Only in an emergency should they be used at all, and the electric heater is by far the best device for such occasions.
It is probably a conservative estimate to say that ninety-five per cent of all the babies occupy a corner of mother's and father's bedroom for the first two or three years. And believing this estimate to be correct, it is advisable to give the matter some consideration. To begin with, a lot of the non-essentials, ruffles and fluffles of the average bedroom, must go. The good father's chiffonier may have to be put in the bath room; heavy floor coverings must be discarded, to be replaced by one or two small, light-weight rugs; wall decorations and the usual bric-a-brac of dressers, tables, etc., should be carefully packed away. In fact, there should be nothing in the room save the parents' bed, dresser (several drawers of which must be devoted to baby's necessities), table, low rocker, a stool, baby's bed and a good big generous screen, made out of a large clothes horse enameled white and filled with washable swiss.
Window draperies must be taken down and packed away, while they are replaced with simple muslin which can go to the laundry twice a month. If it be within the means of the family purse, it is well to renovate the walls just prior to the advent of the little stranger.
And now the baby's bed is placed in the corner most protected from draughts and the glare of the sunlight. If it can be so arranged that baby looks away from the light, and not at it, we are guarding it from defective vision in the future.
Many a beautiful artistic creation so much admired in this world is found to be, on closer inspection, a very ordinary thing which has received an artistic touch; and so, many convenient, sanitary, and beautiful cribs are fashioned from market baskets fastened to tops of small tables whose legs are sawed off a bit; from soap boxes fastened to a frame, and from clothes baskets. A can of white enamel, a paint brush and the deft hand of a merry, cheery-hearted expectant mother can work almost miracles. Remember, please, that all draperies must be washable and attached with thumb tacks so as to admit of easy and frequent visits to the laundry.120
A medium-sized clothes basket will take care of our baby for four or five months. The same general plan for the mattress and bedding is followed as before described.
If necessary—and it usually is, especially during the winter months—a hot-water bottle may be placed underneath the bedding on top of the mattress. This insures a steady, mild, uniform warmth and it not only saves the baby from the danger of being burned, but it also obviates the temporary overheating of the child which usually occurs when the bottle is placed inside the bed, next to the baby. If the bed is properly made—the blankets coming from under the babe up and over—there is little or no need for extra heat for well babies after the first month.
If electric lighting is not an equipment of the home neither gas or oil lamps should be allowed to burn in the room for long periods. For emergency night lighting a well-protected wax candle should be used. However, don't go to sleep and allow a candle to burn unprotected as did one tired, exhausted mother. The father, suddenly aroused from his sleep, saw a large flame caused by the overturning of a wax candle into a box of candles, while the lace drapery of the basinet was within a few inches of the flame and the baby just beyond. Grabbing a pillow he smothered the flames and saved baby and all.
Plenty of fresh air and lots of sunshine should enter baby's room. The large screen amply shields from draughts, and when thus protected there need be no unnecessary concern about cool fresh air, especially after two or three months, as it is invigorating and prevents "catching cold." Warm, stuffy air is devitalizing and even during the early weeks when the fresh air must be warm, an electric fan should be advantageously placed so that many times each day the warm fresh air may be put in motion without creating a harmful draught.121
Warm stuffy air makes babies liable to catch cold when taken out into the open.
Throw open the windows several times each day and completely change the air of baby's room. In the absence of the large screen, a wooden board five or six inches high is fitted into the opening made by raising the lower window sash. Then as the upper sash is lowered the impure air readily escapes while fresh air is admitted.
Make early preparations for bathing the baby in the easiest possible manner; in fact, the young mother should seek to attend to all her duties—the family, the home, and the baby—in the easiest way. For the administration of a bath during the early months, a table is needed, protected by oilcloth on which is placed a roomy bathtub with a folded turkish towel on the bottom for baby to sit on. In addition to the tub, have:
| An enameled pitcher for extra supply of warm water. | A medicine dropper for washing baby's eyes. |
| A small cup for boracic acid solution. | Talcum powder. |
| Castile soap. | Oil or vaseline. |
| A soft wash cloth. | Sterile cotton. |
| Several warmed soft towels. | Tooth picks. |
| A bath thermometer. | A needle and thread for sewing on the band. |
| All of the clean clothing needed. |
See that the bathtub is clean and enamel unbroken, and if it has been used by another babe, freshen it with a coat of special enamel sold for that purpose.
| During the first eight weeks | Temperature 100 F. |
| From two to six months | Temperature 98 F. |
| From six to twenty-four months | Temperature 90—97 F. |
A bath at ninety-eight degrees is a neutral bath, and after the baby is six months and over, the bath may be given at this temperature, and at the close quickly cooled to ninety degrees.122
The nursery should furnish the baby's first protection from contagious diseases. It must be a veritable haven of safety. Therefore, no house work of any kind should be done in the room, such as washing or drying the baby's clothes. The floors and the furniture should be wiped daily with damp cloths. A dry cloth or feather duster should never be used to scatter dust around the room.
All bedding and rugs should receive their daily shaking and airing out of doors, remembering that particles of dust are veritable airships for the transportation of germs. In every way possible avoid raising a dust. So much of the lint which commonly comes from blankets may be avoided with the daily shaking out of doors.
Soiled diapers should not accumulate in a corner or on the radiator; their removal should be immediate, and if they must await a more opportune time, soak them in a receptacle filled with cold water. Even those diapers slightly wetted should never be merely dried and used again, but should be properly washed and dried. No washing soda should be used in the cleansing of diapers—just an ordinary white soap, a good boil, and plenty of rinse water, with drying in the sun if possible. They require no ironing. Hands that come in contact with soiled or wet diapers must be thoroughly cleansed before caring for the baby or preparing his food.
As before mentioned, and it will bear repetition often, all windows and doors must be well screened, for flies and mosquitoes are dreaded foes in any community and in babyland in particular. All used bottles and nipples as well as used cups, pitchers, bits of used cotton, should be removed at once. The washcloth is a splendid harbinger of germs. There should be one for the face, and one for the body and bath, and both should receive tri-weekly boiling. Bath towels should not be used more than twice, better only once.
The technic of bathing, together with the location, furnishings, and cleanliness of the baby's sick room, will be taken up in later chapters.
It is surprising how soon even a young and inexperienced mother will learn to distinguish between the pain cry and the plain cry of her baby; for most crying can easily be traced to some physical discomfort which can be relieved, or to some phase of spoiling and indulgence which can be stopped.
The young baby can neither walk, talk nor engage in gymnastics, except to indulge in those splendid physical exercises connected with a good hearty cry. To be good and healthy, an aggregate of an hour a day should be spent in loud and lusty crying. He should be allowed to kick, throw his arms in the air and get red in the face; for such gymnastics expand the lungs, increase general circulation and promote the general well-being of the normal child. As the child grows older and is able to engage in muscular efforts of various sorts, these "crying exercises" should naturally decrease in frequency and severity. When baby cries, see that the abdominal band is properly applied, that rupture need not be feared.
The sound most welcomed by both doctor and nurse is the cry of the newly born child, for it shows that the inactive lungs have opened up and the baby has begun to use them, for all the time baby was living in the uterine room he did not breathe once, the lungs having been in a constant state of collapse; and not until now, the very moment the air comes in contact with his skin, do the lungs begin to functionate as he emits his first lusty holler.124
The cry is said to be abnormal when it continues too long or occurs too often. It may be strong and continuous, quieting down when he is approached or taken up; or it may be a worrying, fretful cry, a low moan or a feeble whine. And now as we take up the several cries, their description, cause, and treatment, we desire to say to the young mother: Do not yourself begin to fret and worry about deciding just which class your baby's cry belongs to; for help, knowledge, and wisdom come to every anxious mother who desires to learn and who is willing to be taught by observation and experience.
The continuous, fretful cry, accompanied by vigorous sucking of the fists, both of which stop when hunger has been satisfied, is without question the hunger cry.
If this cry is constant with regular feedings, then the quantity of the food must be increased, or the quality improved. The tired, fretful hunger cry must not be neglected; the cause must be removed, for it points to malnutrition.
One day when lecturing at an Iowa chautauqua, I remained in the beautiful park for the noonday meal. It was a warm day and the tables in the well-screened dining tent were filled with mothers who, like myself, preferred the cool shade of the park to the hot ride through the city to the home or hotel dinner. At my table a baby was pitifully crying. The mother had offered the little child seated in a small uncomfortable go-cart, milk, bread, and a piece of cake—all of which were ruthlessly pushed aside. My little son, then only four and a half, said "Mamma, maybe the baby's thirsty," and up he jumped, hurried to the mother's side with his glass of water, saying, "I haven't touched it, maybe the baby's thirsty." The mother brushed the boy aside, saying, "No, I never give the baby water." In spite of the mother's remonstrance, the baby cried on and on, and finally on "trying" the water, the child drank fully one-half the glass and the crying was hushed.125
Babies should be given water regularly—many times every day—from birth, in varying amounts from two teaspoons to one-half cup, according to the age of the child. The water should be boiled for the first few months, and longer if there is any suspicion of impurities.
Milk to the nursing infant is like beefsteak and potatoes to the adult; and many times the milk bottle or the breast is just as nauseating to the thirsty babe, as meat would be to the very thirsty adult whose hunger has previously been fully satisfied.
The babe who is wet, soiled, too hot, or is wrapped too tightly, or who has on a tight, uncomfortable belly band, or whose clothing is full of wrinkles, has only one way to tell us of his discomfort, and that is to cry. It is a fretful cry and should command an immediate investigation as to the possible cause. It takes but a moment to discover a wet diaper; to run the hand up the back under the clothes; to sprinkle with talcum if perspiring; to straighten out the wrinkled clothing; to find the unfastened pin that pricks; or to loosen the tight band. Acquire the art of learning to perform these simple tasks easily, and any or all of these services should be rendered without taking the child from its bed.
Let the child early learn to rest happily and quietly in his own bed. The pillow or mattress may be turned or perhaps the mattress be raised nearer the edge of the basinet. One poor youngster instantly stopped his fretful cry when his mattress was raised four or five inches so he could get the air, at the same time taking him out of his hot room to a cooler room with raised windows. Babies like cold air. They cry when the air is hot, or even warm and close. Every day—rain or shine, wind or sleet—babies should nap out of doors on the porch, in a well-sheltered corner. A screen or a blanket protects from the wind, sleet, or rain; and if the baby's finger tips are warm, you can rest assured the feet and body are warm. Scores of babies will sleep out on the porch, on the protected fire escape, or in a room with opened windows, from one bottle or feeding to another; being aroused at the end of the three or four hour126 interval just enough to nurse, when back they go to their delightful, warm nest in the cool, fresh air to sleep for another period. Babies should never sleep in a room with closed windows.
One of the incidents that surprised me most in my early work with dispensary babies was the utter misconception of the purpose of the belly band. Invariably it was put on so tightly that I could not slip a finger between it and the babe. It is not a surgical instrument, neither is it a truss. These tight belly bands are a source of much fretting and crying.
The little pinched look about the face, the drawing up of the legs, the jerking of the head, arms, or legs, associated with a strong, sharp, unceasing or intermittent cry, demands immediate attention Our first work should be to go about quietly, painstakingly, and systematically to locate the cause of this "cry of pain."
There are often some accompanying symptoms to the cry of pain which demand skilled medical advice and attention, such as the arching of the body backward, the drawing of the head strongly to one side, the inability to use one side of the body, or the presence of fever. There may be an earache, an abdominal complication, or a sore throat, any one of which will be detected by the skilled doctor.
Earache frequently occurs in young babies who have been taken out of doors without proper protection to the ears; or, it may be associated with a cold in the head, which is not detected until the mischief has already been done, while the resulting running ear tells the tale of woeful suffering. Earache must always be thought of as a possible cause when the cry of pain accompanies a cold in the head, and if medical aid is secured early, the abscess may be aborted and the deafness of later years entirely avoided. There is only one home remedy for earache, and that is the application of external heat, either by a hot-water bottle or hot-salt bag. Medical advice should be sought before anything whatsoever is dropped into the baby's ear.127
In this connection should be mentioned the wild cry at night which so often accompanies tuberculosis of the bone. A careful X-Ray examination will reveal the disease, and proper medical measures should be instituted at once. Other fretful night crying will be mentioned further on.
By the frequent repetition of actions, habits are formed. When the baby is two or three days old, he is so new to us and we have waited for him so long, and it is such a great big world that he has come into, that we jump, dance, and scramble to attend to his every need and adequately to provide for his every want. At this very early, tender age whenever he opens his mouth to cry or even murmur—some fond auntie or some overly indulgent caretaker flies to his side as if she had been shot out of a gun, grabs him up and ootsey tootsey's him about as she endeavors to entertain and quiet him. The next time and the next time and the succeeding time he whimpers—like a flash someone dashes to the side of the basket, and baby soon learns that when he opens his mouth and yells, somebody comes. In less than a week the mischief has been done and baby is badly spoiled. No other factor enters so largely into the sure "spoiled" harvest as picking a new baby up every time he cries. Often in the early days some indulgent parent will say, "Oh, don't turn out the light, something might happen to the dear little thing"—and old Mother Nature sees to it that a constant repetition of "leaving the light on" brings its sure harvest of "he just won't go to sleep without the light." And then, "just once" he had the pacifier—perhaps to prevent his crying disturbing some sick member of the family—and so we go on and on. If a thing is bad, it is bad, and a supposedly good excuse will not lessen the evil when the habit has been thus started and acquired.
The rocking of babies to sleep may be a beautiful portrayal of mother love, but we all pity the child who has to be rocked to sleep as much as we do the mother who sits and rocks, wanting, Oh, so much! to do some work or go for a walk—but she must wait till baby goes to sleep.128
And so now we come to the temper cry—that lusty, strong outburst of the cry of disappointment when he finds that all of a sudden people have stopped jumping and dancing for his every whim. The baby is not to blame. We began something we could not keep up, and he—the innocent recipient of all our indulgences—is in no sense at fault. It is most cruel to encourage these habits of petty indulgence, which must cause so much future disappointment and suffering on the part of the little fellow as he begins to grow up.
Nobody is particularly attracted to the spoiled baby. After the over-indulgent parent and caretaker have completed their thoughtless work, they themselves are ashamed of it and not infrequently begin to criticise the product of their own making—the formation of these unpleasant bad habits. More than anything else, the spoiled child needs a new environment, new parents, and a new life.
Seek to find out if possible—and it usually is possible—just what he is crying for. It may be for the pacifier, for the light, or to be rocked, jolted, carried, taken up and rocked at night, or a host of other trifles; and if he is immediately hushed on getting his soul's desire—then we know he is "spoiled."
The unfortunate thing about it all is that the one who has indulged and spoiled the baby usually does not possess the requisite nerve, grit, and will power to carry out the necessary program for baby's cure. And the pity of it all is that overindulgence in babyhood so often means wrecked nerves and shattered happiness in later life. So, fond, indulgent parents, do your offspring the very great kindness to fight it out with them while they are young, even if it takes all summer, and thus spare them neurasthenia, hysteria, and a host of other evils in later life.
This sort of "spoiled baby crying" can be stopped only through stern discipline—simply let the baby "cry it out." The first lesson may require anywhere from thirty minutes to an hour and thirty minutes. The second lesson requires a much129 shorter time, and, in normal babies with a balanced nervous system, a third or fourth lesson is not usually required.
The cry of the severely sick child is the saddest cry of all. The low wail or moan strikes terror to the saddened mother-heart. It is often moaned out when the child is ill with "summer complaint" or other intestinal disturbances. Instant help must be secured, and, if medical help is not obtainable, remember, with but one or two exceptions, you are safe in carefully washing out the bowels, in applying external heat and giving warmed, boiled water to drink.
Another cry which demands immediate attention, and the faithful carrying out of the doctor's orders, is the hoarse, "throaty" cry indicative of croup or bronchitis.
Perhaps the greatest cause of the most crying during infancy, next to that of over-indulgence, is ordinary colic which—
... manifests itself in every degree of disturbance from mere peevishness and fretfulness to severe and intensely painful attacks in which restlessness passes into grunting, writhing, and kicking; the forehead becomes puckered and the face has an agonized expression; the baby tends to scream violently and draws his thighs up against his belly, which will usually be found to be hard and more or less distended.
A colicky baby completely upsets the household and greatly disturbs the mother, who requires both quiet and rest that she may the better produce the life-sustaining stream so much needed for the upbuilding and development of the growing child.
While colic is so often seen in the bottle-fed babe, it often occurs in the breast-fed child, and is usually traceable to some error in the mother's diet or to some other maternal nutritional disturbance. One mother who was sure she had eaten nothing outside the diet suggestions she had received, was requested to130 bring to the office a fresh voiding of her own urine which was found to be highly acid. The administration of an alkaline such as simple baking soda or calcined magnesia to the mother, corrected this acidity, and the colic in the baby entirely disappeared. I recall the case of one mother who ate her dinner in the middle of the day, with a light meal in the evening and thereby stopped the colic in her babe.
Another source of colic in the breast-fed baby is the unclean nipple. The nipples should be washed with soap and water and rinsed in boracic acid solution before each nursing. If the mother worries greatly, or thoughtlessly "gets very angry" just before the nursing hour, there is a substance known as "epinephrin" secreted by the glands located just above the kidneys which is thrown into the blood stream and which raises the blood pressure of the mother and often produces not only colic in the babe, but many times throws him into severe convulsions.
There are many opportunities for colic in the bottle-fed baby; for instance, dirty bottles, dirty nipples, careless cleansing of utensils used in the preparation of baby's food, improper mixtures, too much flour, the wrong kind of sugar, too much cream or too little water—all these things help to produce wind under pressure in the intestine, which is commonly known as colic. Underfeeding or overfeeding, too rapid feeding or too frequent feeding also contribute their mite in producing colic.
As a rule, the bottle-fed child is fed too often. In the new born, the interval between feeds should be three hours from the start; after six months the interval may be lengthened to four hours.
Hiccough—a spasm of the diaphragm—often accompanies colic, and, in the case of infants, is usually due to the swallowing of air or over-filling the stomach; gentle massage, external heat, and a few sips of very warm water usually corrects the condition.131
The chilling of the skin very often produces a temporary intestinal congestion with colic as the result. Cold feet, wet diapers, and loitering at bath are all very likely to produce colic; and when it is thus caused by chilling, quickly prepare a bath at 100 F., and after immersing the child for five minutes, wrap up well in warm blankets.
Those of my mother readers who have electric lights in their home, will find the photophore to be a source of great comfort and convenience; for this simple contrivance is usually able to banish colic in a few moments. The photophore is simply radiant heat—heat plus light (See Fig. 3)—and as this heat is applied to legs and buttocks of the crying child the diaper is warmed, the abdomen relaxes, gas is expelled, intestinal contractions relieved, and the baby is soon fast asleep.
Occasionally with the aid of the photophore, and even without it, the warm two-ounce enema containing a level teaspoon of baking soda and a level teaspoon of salt to a pint of water when allowed to flow into the bowel, will soon bring down both gas and feces to the great relief of the baby. Warm water to drink is also very helpful. Putting the feet in very warm water is also quieting to the crying colicky babe.
It is often necessary in cases of repeated and persistent colic, Do not jolt or bounce the baby, do not carry him about, and don't walk the floor with him.
Heat him up inside and outside, warm his clothing and his bedding, and thus bring about relief without sowing seeds for future trouble—the sorrow of a spoiled child.
One very quiet little baby was one day brought to the dispensary whose mother said: "Doctor, I didn't bring him 'cause he's sick, but 'cause he looks so pale; he's as quiet as a mouse; he never cries any more since I got to giving him medicine." On examination of the baby and on inquiring about the medicine, we found that the baby was dead drunk all the time. Some "neighbor friend" had told the tired out mother, "Give him a teaspoon of whiskey at each feeding and that'll fix him all132 right." If a few more states go dry maybe it will not be so easy for the ignorant mother to dope and drug her helpless baby.
And neither is paregoric to be administered wholesale for colic. It contains an opiate, and should not be given without definite orders from a physician. And so as a parting word on "Why Babies Cry," we ask each mother to run over the following summary of the chapter, and thus seek to find out why her baby cries.
| He is hungry. | He is too cold. |
| He is thirsty. | He is in pain. |
| He has been given a dirty bottle. | He is very sick. |
| His mother has failed properly to cleanse the nipples. | His throat is sore. |
| His food is not prepared right. | His ear aches. |
| His food is too cold. | He has been rocked, carried, or bounced. |
| His bowels are constipated. | He has been given a pacifier. |
| His band is too tight. | He has had too much excitement. |
| His clothes are wrinkled. | His mother has eaten the wrong food. |
| His diaper is wet. | |
| He is too hot. | |
| He wants fresh air. |
Happy is the mother, and thrice blessed is the babe when he is able to enjoy the supreme benefits of maternal nursing. The benefits to the child are far reaching; he stands a better chance of escaping many infantile diseases; the whole outlook for health—and even life itself—is greatly improved in the case of the nursing babe, as compared with the prospect of the bottle-fed child. Maternal nursing lays the foundation for sturdy manhood and womanhood.
Out of every one hundred bottle-fed babies, an average of thirty die during the first year, while of the breast-fed babies, only about seven out of every one hundred die the first year. At the same time, nursing the babe delivers the mother from all the work and anxiety connected with the preparation of the artificial food, the dangers and risks of unclean milk, and the ever-present fear of disease attendant upon this unnatural feeding. The mother who nurses her child can look forward to a year of joy and happiness; whereas, if the babe is weaned, she is compelled to view this first year with many fears and forebodings. Mother's milk contains every element necessary for the growth and development of the child, and contains them in just the proportions required to adapt it as the ideal food for that particular child.
A dirty baby, properly fed, will thrive. A baby deprived of fresh air, but wisely fed, will survive and even develop into a strong healthy man or woman. But the baby raised according to the latest and most approved rules of sanitation and hygiene, if improperly fed, will languish and die.
Outings and Exercise. It is most highly important that the nursing mother should be able thoroughly to digest her food; otherwise the flow of milk is likely to contain irritants that will disturb the baby's digestion, even to the point of making him really sick. In order to avoid these complications, exercise and outings are absolutely essential for the mother. A vigorous walk, gardening, light housework or other light athletics, greatly facilitate digestion and increase the bodily circulation, as well as promote deep breathing, all of which are of paramount importance to a good appetite and good digestion.
The Bowels. The bowels should move regularly and normally once or twice during the twenty-four hours. Unfortunately, this is not usually the case: and in this connection we would refer our reader to the chapter on "The Hygiene of Pregnancy," particularly those sections relative to the care of the bowels, recipes for bran bread, lists of laxative foods and other suggestions pertaining to the hygiene of the nursing mother.
Sleep. Nothing less than eight hours sleep will suffice for the nursing mother, and during the day she should take at least one nap with the baby.
Care of the Skin. Salt-rub baths are very beneficial taken once a week. The daily cold-friction rub described elsewhere, will tone up the system and increase digestion and improve the general well being. The soap wash may be taken once a week. The thorough cleansing of the breasts, and the frequent changing of the undergarments, will help to keep the baby happy; for oftentimes it is the odor of perspiration as well as the smell of soiled clothing that spoils the appetite of the baby, causing it to refuse food.
Recreation. Pleasant diversion is very essential for the mother, and should be indulged in at least once a week. The bedtime hours, however, should not be interfered with and the recreation should be selected with a view to amuse, refresh and create a harmless diversion for the mother's mind. Under no circumstances should the mother settle down to the thought: "No, I can't go out any more. I can't leave my baby." You135 should get away from the baby a short time each day, and go out among your former friends and acquaintances. Many a wrecked home—a shattered domestic heaven—dates its beginnings back to the days when the over-anxious young mother turned her back on her husband and looked only into the face of her (their) child. Nothing should come in between the filial friendship of husband and wife, not even their child. So, dear mother, if you can, go out occasionally, away from the baby, and enjoy the association of your husband and keep in touch not only with his interests, but with the outside world. You will come back refreshed and wonderfully repaid, and the face of the adored infant will appear more beautiful than ever.
The general suggestions on diet which we made to the expectant mother are also valuable for the nursing mother. The food should be appetizing, nutritious, and of a laxative nature. Three meals should be eaten: one at seven a. m., one at one p. m. and one about six-thirty at night, with the heaviest meal usually at one p. m. As the mother usually wakens at five o'clock, or possibly earlier, she should be given a glass of milk, cocoa, or eggnog. If she awakens at six, nothing should be taken until the breakfast, which should consist of a good nourishing meal, such as baked potatoes with white sauce, poached eggs, cereal, milk or cocoa, prunes, figs, or a baked sweet apple, with bread and butter, etc.
From that hour until one p. m. only water is taken, and several glasses are urged during this interval. With nothing between meals but water and a little outdoor exercise, a good appetite is created for the one p. m. meal which should abundantly supply and satisfy the hungry mother; and then again, nothing is to be taken between dinner and supper but water. And after the supper hour, a walk out into the cool night air should be enjoyed with the husband and on going to bed about ten p. m., an eggnog or glass of milk may be taken. At the close of the other meals a cup of oatmeal gruel or milk or any other nourishing liquid may be enjoyed.
The eating of food or the drinking of nourishing drinks136 between the meals not only interferes with digestion and disturbs the mother, but it also upsets the baby; and it is often the reason why the appetite of the mother is so deranged at the meal time, her spirits depressed, and her milk diminished. Plenty of good nourishing food, taken three times a day with an abundance of water drinking between the meals, together with a free happy frame of mind occasioned by the recreation before mentioned, usually produces good milk and plenty of it. A nap between meals will probably produce more milk than eating between meals.
All foods that cause indigestion in the mother or babe should be avoided.
Some mothers continue to eat tomatoes, peaches, sour salads, acid fruits, and it appears in no way to interfere with baby's comfort; but they are the exception rather than the rule. Usually tomatoes, acid salad dressings, and mixed desserts must be avoided. Each mother is a law unto herself. Certainly none of our readers will selfishly continue any food she feels will make her baby cry. All acid fruits, rich desserts, certain coarse vegetables, concoctions of all descriptions such as rarebit, condiments, highly seasoned sauce, etc., should be avoided.
Acid fruitades, such as lemonade, limeade and orangeade, can be taken by a small per cent of nursing mothers; and, since fruit acids are neutralized and alkalized in the process of digestion and assimilation, and since they are the very fruit-drinks we prescribe for patients suffering with an increased acidity, it would appear that they were in every way wholesome for the mother—if they in no way interfere with the baby. Practically, they do as a rule disturb the baby's digestion and should be avoided by those mothers who have found this to be the case.
During the first week of lactation the milk tubes of the breasts very often become blocked and the breasts become engored with milk, this condition being known as "caked137 breasts." At this particular time of the baby's life, he takes little more than an ounce of milk at a feed; so, beside the incoming engorgement of milk, an additional burden is thrown upon the milk tubes of the breasts in that they are not entirely emptied each nursing time by the young infant. When the breasts threaten to "cake," immediate steps must be taken to relieve the condition—to empty the breasts—and this is usually accomplished in the following manner: with hands well lubricated with sweet oil or olive oil the nurse begins gentle manipulation of the breasts toward the nipple in circular strokes, with the result that the milk soon begins to ooze out. This massage should be continued until relief is obtained; or the breast pump may be applied. Hard nodules should not be allowed to form or to remain in the breasts. Hot compresses (wrung from boiling water by means of a "potato ricer") may be applied to the caked breast which is protected from the immediate heat by one thickness of a dry blanket flannel. These hot compresses should be removed every three minutes until three have been applied, then an ice water compress is quickly applied, to be followed by more hot ones and then a cold; and so on, until as many as four sets each have been administered.
Gentle massage may again be administered and it will be found that they empty now with greater ease because of the preceding heat. After the breasts have been emptied, and thoroughly washed with soap suds and carefully dried, they should be thickly covered with cotton batting and firmly compressed against the chest wall by a snug-fitted breast binder, which serves the double purpose of relieving pain by not allowing the breasts to sag downward, at the same time preventing an over-abundant secretion of milk by diminishing the blood supply to the glands of the breast. In case the persistent manipulation of the breast and the use of the breast pump do not relieve the condition, and if the repeated effort day after day seems to avail nothing; then, as a rule, we must look for a breast abscess to follow if the breasts are not immediately "dried up." In all such cases of engorgement, the attending physician should be notified at once.138
The nipple must be kept dry between nursings, which should be limited to twenty minutes. Regularity should be maintained. The nipples should never be touched or handled by hands that have not been scrubbed with soap and a nail brush. During the early nursing days they are wet much of the time and are subject to much stress and strain in the "pulling effort" of the baby, as a result of which they become very tender, chapped, cracked, and often bleed. Allowing the baby to go to sleep with the nipple in his mouth also exposes the nipple to unnecessary moisture which increases the possibility of painful cracking. The pain occasioned by nursing at this time is truly indescribable, and is most often the cause of absolute refusal on the part of the mother to nurse her babe—with the result that it is put on the bottle. Again, the fear and dread of being hurt so often tends to diminish the flow of milk. It is entirely possible so to prepare the nipple for this exposure, during the last months of pregnancy, that all this discomfort and pain may be entirely avoided (See chapter, "The Hygiene of Pregnancy").
Before the mother is put to rest after the birth of the baby the breasts are prepared as follows: A thorough cleansing with soap and water is followed by a careful disinfection with alcohol which leaves the nipple perfectly dry. A soft sterile pad is then applied and held in place by a breast binder. Before and after each nursing the nipple and surrounding area is swabbed with boracic acid (saturated solution) and carefully dried by applying a clean, dry, sterile pad.
Painful cracks and fissures are nearly always due to lack of the care described above, and are almost wholly preventable. When the first crack appears and nursing becomes painful, the baby's mouth should not touch the nipple again until healing has taken place. A thorough cleansing with boiled water should be made and then the sterile nipple shield should be applied through which baby will get abundant satisfaction, while the mother is spared the pain, and the nipple has an opportunity to get well.139
In the case of sore and cracked nipples, thorough cleansing with boiled water and boracic acid solution follows each nursing seance; and, after careful drying, balsam peru—equal parts with glycerine—may be applied with a tiny piece of sterile gauze or cotton; a sterile cotton pad is then applied to each breast which is held in place by a breast binder.
The nipple shield, when employed, is boiled after each nursing and washed in boracic acid solution just before each nursing. The strictest cleanliness must be observed, and then we hope to bring relief and comfort to the mother, and effect the saving of nature's best food for the baby.
Mother's milk—that wonderfully adaptable, ever-changing food, so accurately and scientifically suited to the hourly and daily needs of the growing child—is composed of five different parts, totally unlike in every particular, and each part exactly suited to the needs which it supplies. The cream of the milk, as well as the lactose or sugar, builds up the fatty tissues of the body as well as helps provide the energy for crying, nursing, kicking, etc. The proteins (the curd of the milk) are exceedingly important; they are especially devoted to building up the cells and tissues of the body of the growing child. The salts form a very small part of the baby's food, but an important one, for they are needed chiefly for the bones and the blood. The fats, sugars, proteins, and salts, taken together, form the solids of mother's milk, and are held in solution in the proportion of thirteen parts of solids to eighty-seven parts of water; which so holds these solids in solution that the baby can digest and assimilate these necessary food elements. The mother's milk increases in strength day by day and month by month as the baby grows, and is the only perfect infant food on earth.
Soon after the birth of the baby the wearied mother seeks rest—she usually falls into a quiet, restful slumber; the baby likewise goes to sleep and usually does not awaken for several hours. After six or eight hours the child is put to the breast140 and he begins to nurse at once, without any special help. This first nursing should be discontinued after four or five minutes, while he is put to the other breast for the same length of time.
If there is difficulty in sucking, a bit of milk may be made to ooze out on the clean nipple, while the baby's lips are pressed to it, after which the nurse gently presses and rubs the breasts toward the nipple. After the nursing, the nipples should be elongated, if necessary, by rubbing, shaping, or breast pump.
The baby gets but little nourishment during the first two days, but that which he does get is essential; for the colostrum—the first milk—is highly laxative in nature and serves the important purpose of cleaning out the intestinal tract of that first tarry, fecal residue, the meconium. This early sucking of the child accomplishes another purpose besides the obtaining of this important laxative—it also reflexly increases the contractibility of the muscles of the womb, which is an exceedingly important service just at this time.
Should the mother or caretaker feel that baby will starve before the milk comes, or that it is necessary to provide "sweetened water;" let us assure them that nothing is needed except what nature provides. Nature makes the babe intensely hungry during these first two days, so that he will suck well, and if he is fed sweetened water, gruel, or anything else, he will not suck forcefully; and so nature's plan for securing extra or increased uterine contractions and the stimulation of the breast glands will be seriously interfered with.
As soon as the new born babe is washed and dressed he is given two teaspoons of warmed, boiled water; and this practice is continued every two hours during the day, until as much as two to four ounces of unsweetened water is taken by the tiny babe during the twenty-four hours. Inanition fever—the fever that sometimes follows a failure to give water to the new born infant—is thus avoided. The bottle from which the water is given should be scalded out each time, the nipple boiled, and just before the "water nursing" the nipple should be swabbed with boracic acid solution.141
From earliest infancy the baby should be nursed by the "clock," and not by the "squawk." Until he reaches his sixth-month birthday, he is fed with unerring regularity every three hours during the day. Asleep or awake he is put to the breast, while during the night he is allowed to sleep as long over the three-hour period as he will. Babies are usually nursed at night: during the early weeks, at nine o'clock in the evening, at midnight, and at six o'clock in the morning. After four months all nursing after ten p. m. may be omitted.
The baby is ordinarily allowed to remain at the breast for about twenty minutes. He may often be satisfied with one breast if the milk is plentiful; if not, he is given both breasts; and may we add the following injunction? insist that nothing shall go into your baby's mouth but your own breast milk and warm or cool-boiled water; no sugar, whiskey, paregoric, or soothing syrup should be given, no matter how he cries. Never give a baby food merely to pacify him or to stop his crying; it will damage him in the end. More than likely he is thirsty, and milk to him is what bread and meat are to you, neither of which you want when you are thirsty.
A perfectly comfortable position during nursing for both mother and babe is necessary for satisfactory results. During the lying-in period the mother should rest well over on her side with her arm up and her hand under her head, the other hand supports the breast and assists in keeping the nipple in the baby's mouth, as well as preventing the breast from in any way interfering with baby's breathing. A rolled pillow is placed at the mother's back for support.
After the mother leaves the bed, she will find a low chair most convenient when nursing the baby, and if an ordinary chair be used, she will find that a footstool adds greatly to her comfort. Once during the forenoon and once during the afternoon the nursing mother will find it a wonderful source of rest and relaxation if she removes all tight clothing, dons a comfortable wrapper, and lies down on the bed to nurse her babe;142 and as the babe naps after the feed, she likewise should doze and allow mother nature to restore, refresh, and fit her for restful and happy motherhood.
Worry, grief, fatigue, household cares, loss of sleep, social debauches, emotional sprawls—all debilitate the mother, and usually decrease the flow of milk.
Overheating, irritability, and sudden anger, almost invariably tend to raise the blood-pressure, which means the entry into the blood stream of an increased amount of epinephrin, which disturbs the baby greatly, often throwing him into convulsions or other sudden, acute illness.
Menstruation often interferes with the nursing mother, the milk becoming weaker at this time; however, if the infant continues to gain and the mother feels comparatively well, no attention need be paid to this fact.
Another pregnancy demands a drying up of the breast at once, as the tax is too great on the mother.
The stools of the breast-fed baby do not require as much attention as those of the bottle-fed child. In cases of constipation, after four months, from one teaspoon up to one-half cup of unsweetened prune juice may be given one hour before the afternoon feed.
In instances of colic with signs of fermentation in the stool, the mother may take several doses (under her physician's orders) of common baking soda; or, if she is constipated, calcined magnesia will usually right the condition. Nature's mother milk is so beautifully adapted to the baby's needs that it is the rule for baby to have perfectly normal stools.
A happy baby is a satisfied baby. He lies quietly in a sleepy, relaxed condition if he has enough to eat, provided he is otherwise comfortable and dry. He awakens at the end of two hours and perhaps cries; but plain, unsweetened, warm, boiled water143 quenches his thirst, and he lies content for another hour, when he is regularly nursed. He gains on an average of about one ounce a day.
Constant discomfort, vomiting, fretful crying, passing and belching of gas, colicky pain, disturbed sleep, greenish stools with mucus, are among the more prominent earmarks of unsuccessful nursing. These symptoms appearing in a pale, flabby, listless, indifferent or cross baby, with steady loss of weight continued over a period of three or four weeks, point to "nursing trouble;" which, if not corrected, will lead to that much dreaded infantile condition—malnutrition.
Bolting of food or overeating results in vomiting and gas, and thus interferes with normal nursing, as also may tongue-tie. A condition in the mouth, medically known as "stomatitis," and commonly known as "thrush," often gives rise to a fretful cry when nursing is attempted. In the first place, the baby cannot "hold on" to the nipple; while, in the second place, it hurts his inflamed mouth when he makes an effort to nurse.
Long continued nursing covering three-fourths of an hour or more, seizing of the nipple for a moment and then discarding it, apparently in utter disgust, are the earmarks of very scanty milk supply and should receive immediate attention.
Believing that many more mothers than do so should nurse their babies, we have carefully tabulated a number of aids to the milk supply, which we hope will be most earnestly tried before the baby is taken from the breast—for so many, many more bottle-fed babies die during the first year than the breast fed. The dangers of infection, the worry of the food preparation, the uncertainty of results, all call for a most untiring effort on the part of every doctor, nurse, and mother, in their endeavors to secure maternal nursing. The following is a summary of "aids to the milk supply:"
1. Regular periodical sucking of the breasts from the day of baby's birth.144
2. Systematic applications of alternate hot and cold compresses, followed by massage to the breasts.
3. Three good nourishing meals each day, eaten with merriment and gladness of heart.
4. A glass of "cream gruel," milk, cocoa, or eggnog at the close of each meal, with a glass just before retiring.
5. Three outings each day in the open air.
6. Nurse the baby regularly and then turn its care over to another, you seek the out of doors and engage in walking, rowing, riding and other pleasurable exercise.
7. Take a daily nap.
8. You can bank on fretting and stewing over the hot cook stove to decrease your milk. It seldom fails to spoil it.
9. Regular body bathing, with cold friction rubs to the skin.
10. A happy, carefree mental state. Nothing dries up milk so rapidly as worry, grief, or nagging.
11. The administration, preferably in the early days, of desiccated bovine placenta; although it may be given at any time during the period of nursing.
As much as we desire maternal nursing for the babe, there do occur instances and conditions which demand a change to artificial feeding, such as the following:
When a maternal anesthetic is to be administered, or in case of inflammation of the breast or during a very short illness not covering more than two or three days, then the breast pump may be used regularly every three hours to both breasts; the145 baby may be artificially fed and then returned to the breast after the effects of the anesthetic has worn off or the temperature has been normal for twenty-four hours.
There may also appear definite indications in certain children which make it imperative that the nursing child should early be weaned. These manifestations of disordered nutrition and failing health admonish us to put the baby on properly modified milk, or to transfer it to a wet nurse.
These conditions are:
1. Progressive loss in weight.
2. A bad diarrhea of long standing; one which does not yield to the usual remedies, at least not as long as the baby continues to feed from the breast. These diarrheas are especially serious when accompanied by a steady loss in weight.
3. Excessive vomiting accompanied by progressive loss in weight.
Because of the rarity of good, healthy wet nurses, it is always better to attempt to feed the baby with scientifically modified milk (not proprietary foods), good, clean, cow's milk properly modified to suit the weight and age of the child. We put weight first, for we prepare food for so many pounds of baby rather than for the number of months old he is.
If modified food has failed and the best specialist within your reach orders a wet nurse; she must have the following qualifications:
If an unmarried mother of her first child is engaged as a wet nurse, she should not be "stuffed" or allowed to overeat, which is commonly the result of moving her from her lower life into more comfortable surroundings, or given ale or beer to increase her milk. She should continue her normal eating, take light exercise, which does not mean the scrubbing of146 floors or doing the family washing, and live under the same hygienic regime outlined for the nursing mother. Should she be the mother of the second or third illegitimate child, then she is quite likely to be mentally deficient and she should not be engaged. Her own babe will have to be fed artificially as very few mothers can endure the strain of two suckling children.
The baby's own mother should keep general supervision and not turn her babe entirely over to the care of the wet nurse. Remember always that no one in the wide world will ever take the same mother interest in your offspring that can spring from your own mother heart.
In taking up the subject of the bottle-fed baby, we must repeat that the only perfect baby food on earth is the milk that comes from the breast of a healthy mother.
But sudden illness, accident, chronic maladies, or possibly the death of the mother, often throw the helpless babes out into a world of many sorts and kinds of artificial foods—foods that are prepared by modifying cow's, ass', or goat's milk; foods arranged by the addition to the milk of various specially prepared cereals, albumens or malted preparations, otherwise known as "proprietary foods." We shall endeavor, then, in this chapter and in that on "the feeding problem," to lay down certain general suggestions to both the nurse and the mother, which may assist them in their effort to select the food which will more nearly simulate nature's wondrous mother-food, and which will, at the same time, be best suited to some one particular baby.
The normal baby, from birth to six months, should receive properly prepared nourishment every three hours, beginning the day usually at six a. m., the last feeding being at nine p. m. During the early weeks an additional bottle is given at midnight, but this is usually discarded at four months, at which time the last feeding should be given at about ten instead of at nine at night.
Should the baby continue to awaken during the night before six in the morning, unless he is under weight, a bottle of warm, boiled, unsweetened water should be given.148
The quantity of food to be given is always determined by the size of the baby's stomach, which, of course, depends somewhat upon the age of the child; for instance, the stomach of the average baby one week old holds about one ounce, while at the age of three months the stomach holds five ounces; so it would not only be folly to give two ounces at one week and seven ounces at three months, but it would also be very detrimental to the babe, causing severe symptoms due to the overloading of the stomach.
Careful study of the size of the stomach at different ages in infancy, together with the quantity of milk drawn from the breast by a nursing baby, has led to the following conclusions regarding the capacity of the baby's stomach:
| AGE | QUANTITY |
| 1—4 weeks | 1—2 ounces |
| 4 weeks—3 months | 2½—4 ounces |
| 3 months—6 months | 4—6 ounces |
| 6 months—1 year | 6—8 ounces |
It is highly important that the day's feedings be kept in a cold place, free from the odors of other foods as well as free from dust, flies, and filth. In order that this may be accomplished, the well-protected bottles, each containing its baby-meal, are placed in a covered pail containing ice and water. This covered receptacle is now put in an ice box; and, in order that our most economical reader—one who may feel that she cannot afford to keep up the daily expense of the family refrigerator—may herself prepare a simple home refrigerator, the following directions are given (Fig. 9).
Procure a wooden box about eighteen inches square and sixteen or eighteen inches deep and put four inches of sawdust into the bottom; now fill in the space between a ten-quart pail, which is set in the middle of the box with more sawdust. A cover for the box is now lined with two or three inches of newspaper, well tacked on, and is fastened to the box by hinges. We are now ready for the inside pail of ice, into which is carefully placed the well-protected bottles of milk, all of which is then set into the ten-quart pail in the box. Five cents worth of ice each day will keep baby's food cool, clean, and provide protection against the undue growth of germs.149
At each feeding hour, one of baby's bottled meals is taken from the ice box and carefully dipped in and out of a deep cup of hot water. A very convenient receptacle is a deep, quart aluminum cup, which may be readily carried about. The hot water in the cup should amply cover the milk in the bottle (Fig. 10).
To test the warmth allow a few drops to fall on the inner side of the arm, where it should feel quite warm, never hot. A baby's clean woolen stocking is now drawn over the bottle, which keeps it warm during the feeding. No matter how great the danger of offending a fond grandparent or a much adored friend never allow anyone to put the nipple in her mouth to make the test for warmth of baby's food.
There are many contrivances, both electrical and alcoholic, for heating baby's bottle, many of which are both convenient and inexpensive.
And now we realize that we are about to advise against the time-honored injunction which has been handed down from "Grandma This" and "Mother That" to all young mothers who have lived in their neighborhoods: "My dear young mother, if you can't nurse your precious infant, you can at least 'mother it' at the nursing time by holding it in your arms and gently rocking it to and fro as you hold the bottle to its lips." This so-called "mothering" has resulted in regurgitation, belching, and numerous other troubles, as well as the formation of the "rocking habit."
A young mother came running into my office one day saying: "Doctor, it won't work, the food's all wrong; my baby is not151 going to live, for he throws up his food nearly all the time." We arranged to be present when the next feeding time came and watched the proceedings. A dear old friend had told her "she must 'mother' her baby at the nursing time," and so she had held the child in a semi-upright position as she endeavored to hold the bottle as near her own breast as was possible. The hole in the nipple was a bit large, which occasioned the subsequent bolting of the food, and then to continue the "mothering" she swayed him to and fro, all of which was interrupted suddenly by the vomiting of a deluge of milk.
I drew the shade in an adjoining room, opened the windows, and into a comfortable carriage-bed I placed the baby on his side. Seating myself beside him I held the warm, bottled meal as he nursed. Several times I took it from his mouth, or so tipped it that "bolting" was impossible. Gradually, carefully, and slowly, I took the empty bottle away from the sleepy babe, and as I closed the door the mother said in anxious amazement: "He won't forget I'm his mother if I don't hold152 him while he nurses?" You smile as I smiled at this girl-mother's thought; but, nevertheless there are many like her—anxious, well-meaning, but ignorant.
The infant stomach is little more than a tube, easily emptied if the baby's position is not carefully guarded after nursing. No bouncing, jolting, patting, rocking, or throwing should take place either just before, during, or immediately after meals.
From twelve to twenty minutes is long enough time to spend at a bottle meal. The nipple hole may have to be made larger, or a new nipple with a smaller hole may have to be purchased. When new, you should be able to just see a glimmer of light through the hole, and if the infant is too weak to nurse hard, or the hole too small, it may be made larger by a heated hatpin run from the inside of the nipple out; great care must be taken, else you will do it too well. If the nipple hole is too large, bolting is the sure result; while too small a hole results in crying and anger on the part of the hungry child, because he has to work too hard to get his meal.
We have seen some mothers, in their anxiety to prevent the sucking in of air from the emptied bottle, rush in and jerk the nipple from the going-to-sleep babe so forcibly that all thoughts of sleep vanished and a crying spell was initiated. The tactful mother is the quiet one who slowly, quietly, draws the empty bottle with its "much loved nipple" from the lips. If you observe that the babe is going to sleep, with an occasional superficial draw at the nipple, wait a moment; he will drop it himself, and you can pick it up as you quietly leave the room. In all instances, whether it be indoors or out of doors, arrange the babe in a comfortable sleeping position, remembering that nursing is warm exercise and the babe gets uncomfortably sweaty if overbundled, especially about the head and neck. No one should unnecessarily touch the babe immediately after feeding; even his diaper may be changed without awakening him while he is thus lying quietly in his bed.153
The three-hour interval is reckoned from the beginning of the meal, and not from its close. More than two hours is spent in the stomach digestion, and any food or sweetened water which may enter between meals only tends to cause indigestion and other disturbances. And that this important organ may have a bit of rest, we fix the interval at three hours, which in our experience and that of many other physicians, has yielded good results. As a rule we have no regurgitation and no sour babies on the three-hour schedule. Sick babies, very weak babies, and their feeding time, will be discussed in a later chapter.
At six months, and often as early as four, in cases of constipation, unsweetened, well-strained prune juice may be given, beginning with one-half teaspoon one hour before the afternoon feed and increasing it daily until two tablespoons are taken. At six months, both orange juice and vegetable broths are given, whose vegetable salts add a very important food element to the baby's diet—an element which our grandmothers thought could only be obtained through the time-honored "bacon rind" of by-gone days.
Orange juice is also unsweetened and well strained, and is administered in increasing amounts, beginning with one-half teaspoon one hour before the afternoon feeding, until the juice of a whole orange is greedily enjoyed by the time of the first birthday. The vegetable juices are obtained from cut-up spinach, carrots, tomatoes, and potatoes, strained, with a flavor of salt and onion—really a bouillon—and is given just before the bottle at the six p. m. feeding. They are also begun in teaspoon amounts.
Baby travel should be reduced to a sheer necessity; never should the babe be subjected to the exposure of disease germs, the change of food, the possibilities of draughts and chilling, for154 merely a pleasure trip—the risks are too great and the possibilities of future trouble too far reaching.
If you are in touch with the milk laboratory of a large city, you will find that they make a specialty of preparing feedings which are good for a number of days for the traveling baby, and we strongly advise that their preparations be accepted; but in the event of not being in touch with such a laboratory we suggest the making of a carrying ice-box covered with wicker, which must be kept replenished with ice. Food kept in such a device may be kept fresh for twenty-four to forty-eight hours. Plans other than the laboratory preparations or the ice-box are risky, and should not be depended upon.
Many of our railway dining cars now pick up fresh, certified milk at stations along the line for use on their tables, and where such is the case fresh preparations of milk may be made on a trans-continental trip by the aid of an alcohol stove. Malted milk may also be used, provided you have accustomed the baby to its use a week before leaving home, by the gradual substitution of a fourth to a half ounce each day in the daily food; all of which, of course, should be done under your physician's direction.
If possible, leave baby at home in his familiar, comfortable environment in the care of a trained nurse and a trusted relative, and under the supervision of the baby's own physician. He is much better off, much more contented, and we are all aware of the fact that contentment and familiarity of sights and people promote good appetite, good digestion, and happiness—the very essentials of success in baby feeding. We speak touchingly and sympathetically to the mother who must leave her babe; and likewise we wish to cheer her as we remind her that by wireless messages and night letters it is possible to keep in touch with loved ones though a thousand miles away.
The sanitation and modification of cow's milk, as well as stools, etc., are taken up in later chapters.
1. Never play with a baby during or right after a meal.
2. Lay the baby on his side when nursing the bottle.155
3. Three full hours should intervene between feedings.
4. Don't give the food too hot—it should just be warm.
5. Make the test for warmth on the inner side of your arm.
6. Give a drink of water between each meal if awake.
7. Never save the left-overs for baby.
8. If possible, give three feedings each day in the cool air, with baby comfortably warm.
9. Do not jump, bounce, pat, or rock baby during or after meals.
10. Never coax baby to take more than he wants, or needs.
11. No solid foods are given the first year.
12. Orange juice may be given at six months; while, after four months, unsweetened prune juice is better than medicine for the bowels.
Cow's milk, like mother's milk, is made up of solids and water. In a previous chapter we learned that in one-hundred parts of mother's milk, eighty-seven parts were water and thirteen parts were solid. These thirteen parts of solids consist of sugar, proteins, and salts; this is likewise the case with cow's milk, except that in the case of the cow's milk, the sugar is decreased while the proteins are increased as will be noted by the accompanying comparative analysis:
| Fat | % 4.00 |
| Sugar | 7.00 |
| Proteins | 1.50 |
| Salts | 0.20 |
| Water | 87.30 |
| ——— | |
| % 100.00 |
| Fat | % 4.00 |
| Sugar | 4.50 |
| Proteins | 3.50 |
| Salts | 0.75 |
| Water | 87.25 |
| ——— | |
| % 100.00 |
Mother's milk is absolutely sterile, that is, free from the presence of germs; on the other hand, cow's milk is anything but sterile—the moment it leaves the udder it begins to accumulate numerous bacteria, all of which multiply very rapidly.157 Cow's milk is generally twenty-four to forty-eight hours old before it can possibly reach the baby. It is just as important to keep in mind these facts of milk contamination—dirt, filth, flies, and bacteria—as it is to plan for the modification of cow's milk for the purpose of making it more nearly resemble mother's milk. While mother's milk has about the same percentage of fat as cow's milk, it is almost twice as rich in sugar, and has only one-fourth to one-third as much protein. This protein is vastly different from that found in cow's milk, which you recall has a tough curd, as seen in cottage cheese. While mother's milk contains a small amount of casein similar to that found in the cheese of the cow's milk, the principal protein constituent is of another kind (lactalbumin), and is much more easy of digestion than the casein of cow's milk.
This is a most important point to remember, because the baby's stomach is not at first adapted to the digestion of the heavier and tougher protein curds of cow's milk. It requires time to accustom the infant stomach to perform this heavier work of digestion. There are a number of factors which must be borne in mind in the modification of milk, whether it be cow's milk, or goat's milk (for many European physicians use goat's milk entirely in the artificial feeding of infants): namely, the cleanliness of the milk, the acidity of milk, the difference in the curd, the percentage of sugar, and the presence of bacteria.
In the modification of cow's milk, sugar must be added to make up for the sugar which is decreased when the water was added to reduce the protein. There are several sorts of sugar used in the modification of milk. These sugars are not added to sweeten the milk alone, but to furnish a very important element needed for the growth of the baby. Sugar is the one element which the infant requires in the largest amount.
Milk sugar is probably most universally used in the modification of milk, but a good grade of milk sugar is somewhat expensive, costing from thirty to sixty cents a pound, and this places it beyond the reach of many mothers. It is added to158 the food mixtures in the proportion of one ounce to every twenty ounces of food. Cane sugar (table sugar) may also be used, but it must be clean and of good quality. It is used in rather less quantity than that of milk sugar, usually from one-half to one-third of an ounce by measure to each twenty ounces of food. Dextri-maltose (malt sugar) is very easy of digestion and may be used in the modification of milk. Maltose seems to help the children to gain more rapidly in weight than when only milk or cane sugar is used. It is also exceedingly useful in constipation, as its action is more laxative than any of the other sugars; but it should not be given to children who vomit habitually or have loose stools.
Like mother's milk, the cow's milk is neutral as it comes from the udder; but, on standing, it quickly changes, soon becoming slightly acid, as shown by testing with blue litmus paper. In fact, what is known as ordinarily fresh milk, if subjected to the litmus paper test, always gives an acid reaction. This acidity is neutralized by adding lime water to the formula in the proportion of one ounce to each twenty-ounce mixture. Ordinary baking soda is sometimes prescribed by physicians in place of the lime water. In the event of obstinate constipation, milk of magnesia is sometimes added to the day's feedings.
There may be procured in any large city an instrument called the cream gauge, which registers approximately (not accurately) the richness of milk. Some milk, even though rich, parts with its cream very slowly; while some poor milk allows nearly all the cream quickly to rise to the surface. We know of no way for the mother to determine the amount of cream (without the cream gauge) except by the color and richness of the milk. In cities it is very convenient to send a specimen of the milk to the laboratories to be examined by experts, who will gladly render a report to both physician and mother.
The lactometer is a little instrument used to estimate the specific gravity of milk. An ordinary urinometer such as used 159by physicians in estimating the specific gravity of urine may also be used. The specific gravity of cow's milk should not register below 1028 or above 1033.
Milk from a single cow is not to be desired for baby's food because of its liability to vary from day to day, not to mention the danger of the cow's becoming sick. Authorities have agreed that herd milk of Holstein or ordinary grade cows is best for infant feeding. This mixed-herd milk contains just about the proper percentage of fat; whereas, if Jersey milk must be used, some of the cream should be taken away. Our milk should come from healthy cows which have been tested for tuberculosis at least every three months.
Annatto is sometimes added to milk to increase its richness of color. To test for annatto proceed as follows: To a couple of tablespoons of milk add a pinch of ordinary baking soda. Insert one-half of a strip of filter paper in the milk and allow it to remain over night. Annatto will give a distinct orange tint to the paper. The commonly used milk preservatives are boracic acid, salicylic acid, and formaldehyde, any of which may be readily detected by your health officials.
In close proximity to most large cities there is usually to be found one or more sanitary dairies. It is a joy indeed to visit a farm of this kind with its airy stables and concrete floors, which are washed with water coming from a hose. The drainage is perfect—all filth is immediately carried off (Fig. 11). The cows are known to be free from tuberculosis, actinomycosis (lumpy jaw), and foot and mouth disease. The milkmen on this farm wear washable clothes at the milking time, and their hands are painstakingly cleansed just before the milking hour. Previous to the milking the cattle have been curried outside the milking room and their udders have received a careful washing. The milkman grasps the teat with clean hands, while the milk is allowed to flow through several thicknesses of sterilized gauze into the sanitary milking pail. This milk is160 at once poured into sterile bottles, is quickly cooled and shipped in ice to the substations where the delivery wagon is waiting. In the ideal delivery wagon there are shallow vats of ice in which the bottles are placed, thus permitting the milk to reach the baby's home having all the while been kept at a temperature just above the freezing point.
And why all this trouble? Why all this worry over temperature and cleanliness? Babies were not so cared for in the days of our grandmothers. The old-fashioned way of milking the cows with dirty clothes and soiled hands, while cattle were more or less covered with manure, with their tails switching millions of manure germs into the milking pail, produced a milk laden not only with manure germs—the one great cause of infantile diarrhea—but also swarming with numerous other mischief making microbes. Even tuberculosis, that much dreaded disease germ of early infancy, may come from the dairy hands as well as from infected cows.
There used to be many dairymen like the old farmer who, when interrogated by the health commissioner concerning the cleanliness of his milk, laughed as he reached down into the bottom of a pail of yellow milk and grabbing up a handful of manure and straw, said: "That's what makes the youngsters grow." But it does not make them grow; it often causes them to die, and even if they do live, they live in spite of such contaminated food, for the germ which is always found in the colon of the cow (coli communis), probably kills more babies every year than any other single thing.
It is possible to reduce the growth of these germs by keeping the milk at a very low temperature from the time it leaves the cow until the moment it gets to the home refrigerator. Those which survive this process of refrigeration may be quickly rendered harmless by pasteurizing or sterilizing at the time of preparing baby's food.
In the absence of the modern sanitary dairy, we would suggest that the milk supply be improved by giving attention to the following:
The cattle should be tested for tuberculosis every three months. The walls of the cowhouse should be whitewashed161 three times a year. The manure should be stored outside the barn. The floor of the cowhouse should be sprinkled and swept each day. The cattle should be kept clean—curried each day, and rubbed off with a damp cloth before milking. The udders should be washed before each milking. The milker can wear a clean white gown or linen duster which should be washed every two days, while his hands should be washed just before the milking. The milking pail should be of the covered sanitary order. The barn should be screened.
Immediately after leaving the cow, the milk should be cooled to at least 45 F. It should at once be put into bottles that have been previously sterilized and then be tightly covered, and should be kept in ice water until ready for consumption. No matter how carefully the milk is handled, it is infected with many bacteria, but if it is quickly cooled, the increase of the bacteria is greatly retarded. Under no circumstances buy milk from a grocery store out of a large can. Go to your health officer and encourage him in his campaign for sanitary dairies and certified milk.
Such milk as we have described under the head of sanitary dairies, when it has been tested by the board of health and has received the approval of the medical profession, is known as "certified milk;" and, although the price is usually fifteen to twenty cents a quart, when compared with the cost of baby's illness it will prove to be cheaper than the dirty milk which sickens and kills the little folks.
There is no doubt that the increased use of "certified milk" has been a great factor in the reduction of deaths from infant diarrhea in recent years.
When certified milk cannot be had, it is absolutely dangerous to give raw, unboiled, or unpasteurized milk to the baby, particularly in warm weather; for the countless millions of manure germs found in each teaspoon of ordinary milk not only disturbs the baby's digestion, but actually makes him sick, causing162 colic, diarrhea, and cholera infantum. The only way this milk can be rendered safe is by cooking it—actually killing the bacteria. This process of boiling, however, does not make good milk out of bad milk nor clean milk out of that which is dirty, it simply renders the milk less dangerous.
There are two methods of killing bacteria—sterilization and pasteurization. By sterilization is meant the process of rendering the milk germ free by heating, by boiling. Many of the germs found in milk are comparatively harmless, merely causing the souring of milk; but other microbes are occasionally present which cause serious diseases, such as measles, typhoid and scarlet fever, diphtheria, tuberculosis, and diarrhea. It is always necessary to heat the milk before using in warm weather, and during the winter it is also important when infectious or contagious diseases are prevalent.
Milk should be sterilized when intended for use on a long journey, and may be eaten as late as two or three days afterward.
To sterilize milk, place it in a well-protected kettle and allow to boil for one hour and then rapidly cool. This process renders it more constipating, and for some children many of its nutritive properties seem to be destroyed, as scurvy is often the result of its prolonged use. When a child must subsist upon boiled milk for a long period, he should be given the juice of an orange each day. Children are not usually strong and normal when fed upon milk of this character for indefinite periods. All living bacteria (except the spores or eggs) may be destroyed by boiling milk for one or two minutes.
When baby is to use the milk within twenty-four hours, "pasteurization" is better than boiling as a method of destroying microbes.
There are many pasteurizers on the market which may be depended upon, among which are the Walker-Gordon Pasteurizer, and Freeman's Pasteurizer; but in the absence of either of these pasteurization may be successfully accomplished by the following method:163
On the bottom of a large kettle filled with cold water, place an ordinary flatiron stand upon which is put a folded towel. On this place the bottle of milk as it comes from the dairyman, with the cap of the bottle loosened. The cold water in the kettle should come up to within an inch of the top of the bottle of milk. Heat this water quickly up to just the boiling point—until you see the bubbles beginning to rise to the top. The gas is then turned down or the kettle is placed on the back of the range and held at this near-boiling point for thirty minutes, after which it is taken to the sink and cold water is turned into the water in the kettle, until the bottle of milk is thoroughly cooled. It is now ready to be made up into the modified food for baby.
Never let pasteurized milk stand in the room, nor put it near the ice when warm. It must be cooled rapidly, as described above; that is, within fifteen or twenty minutes.
The "spores" of the milk are not killed by pasteurization and they hatch out rapidly unless the milk is kept very cold, and, as already stated, it should be used within twenty-four hours after pasteurization.
The certified milk or the ordinary milk that has been delivered to your home and is to be used without pasteurization or sterilization, should receive the following care:
1. It should be placed at once in a portion of the ice box that is not used to store such foods as radishes, cabbage, meats or any other open dishes of food whose odors would quickly be absorbed by the milk. The milk should never be left standing on the doorsteps in the sun, for many reasons: the sun heats the milk, encourages the growth of bacteria, and a passing cat or dog, whose mouth often contains the germs of scarlet fever, tonsilitis, and diphtheria, should it be hungry, laps the tops of the bottles, particularly in the winter when the cream has frozen and is bulging over the edge.
2. It should never be kept in the warm kitchen, as when visiting her sick baby we discovered one young mother doing. In answer to my question, she explained; "Doctor, we do not164 take ice in the winter time, everything is ice outdoors, so I just set the bottle outside the window bringing it in whenever I need to give the baby some food. I forget to put it out sometimes, but really now, does it matter?" It really matters much, for you see, reader, the milk is first freezing then thawing and it is rendered entirely unfit for the baby.
3. Milk should be kept covered and protected from dust and flies; it should be kept in glass jars which have been sterilized by boiling before being filled, and then placed in the refrigerator. If the milk is sour, or if there is any sediment in the bottle, it is unfit for baby's use.
In a previous chapter it was found from comparing the analysis of mother's milk with that of cow's milk, that they widely differed in the proteins and sugar. The art of so changing cow's milk that it conforms as nearly as is possible to mother's milk is known as "modification." Where protein, sugar, and fat are given in proper amounts, healthy infants get along well; but when either the fats or proteins are given in excess, or when the digestion of the child is deranged, there is often no end of mischief.
There are two groups of milk formulas that are useful. First, those in which the fats and proteins are about the same, known as "whole milk," or "straight" milk mixtures; second, those in which the fats are used in larger proportions than proteins, and known as "top milk"—milk taken from the upper part of the bottle after the cream has risen. And since the larger proportion of babies take the lower fats or "whole milk" formulas, and seem to get along better than the babies who have the "top milk" formulas, we will first take up the consideration of the modification of whole milk.
To begin with, everything that comes in contact with the preparation of baby's food must be absolutely clean. The table on which the articles are placed, and any towel that comes in contact with the articles or the mother's hands, or those of the nurse, must be thoroughly scrubbed.
There is only one way to prepare the utensils that are to be used in making the baby's food, and that is to put them in a large kettle and allow them to boil hard for fifteen minutes166 just before they are to be used. The articles needed are (Fig. 12):
| 1. As many bottles as there are feedings in one day. | 10. A bottle of lime water. |
| 2. A nipple for each bottle. | 11. A fine-mesh, aluminum strainer. |
| 3. Waxed paper for each bottle top. | 12. A square of sterile gauze for straining the food (should be boiled for fifteen minutes with the utensils). |
| 4. Rubber bands for each bottle. | 13. One plate, and later a double boiler (14). |
| 5. A two-quart pitcher. | 15. The sugar. |
| 6. A long-handled spoon for stirring the food. | 16. The milk. |
| 7. A tablespoon. | 17. Ready for the ice box. |
| 8. A fork. | 18. Refrigeration. |
| 9. An eight-ounce, graduated measuring glass. |
There is but one bottle which can be thoroughly washed and cleaned, and that is the wide-mouthed bottle. It should hold eight ounces and should have the scale in ounces blown in the side (Fig. 10). The nipple for this bottle is a large, round breast from which projects a short, conical nipple, which more nearly resembles the normal breast than do the old-fashioned nipples so frequently seen on the small-necked nursing bottles. There is a great advantage in this, in that the baby cannot grasp the nipple full length and thus cause gagging. These bottles and nipples are known as the "Hygeia," and have proven to be a great source of comfort to the baby as well as to the mother or nurse whose duty it is to keep them clean. There are a number of other nursing bottles on the market, which, if they are used, must be thoroughly cleansed with a special bottle brush each day. The neck is small and the nipple is small and great care must be taken in the cleansing of both of them.167
When there is a bottle for each individual feeding in the day, immediately after each nursing both bottle and nipple should 168be rinsed in cold water and left standing, filled with water, until the bottles for one day's feeding have all been used. The nipples should be scrubbed, rinsed, and wiped dry and kept by themselves until their boiling preparation for the following day's feeding.
If the same bottle is to be used for the successive feedings during the day, it should be rinsed, washed with soap and water, and both bottle and nipple placed in cold water and brought quickly to the boiling point and allowed to boil for fifteen minutes. No bottles or nipples must ever be used after a mere rinsing; boiling, preceded by a thorough washing in soap and water, must take place before they are used a second time.
New nipples are often hard and need to be softened, which is readily done by either prolonged boiling or rubbing them in the hands.
All new bottles should be annealed by placing them on the stove in a dishpan of cold water and allowing them to boil for twenty minutes, and then allowing them to remain in the water until they are cold. When bottles are treated in this manner they do not break so readily when being filled with boiling water or hot food.
In a large preserving kettle place all the utensils needed in the preparation of the food—pitcher, spoon, fork, measuring glass, bottles, nipples, cheesecloth for straining, agate cup, wire strainer, in fact everything that is to be used in the preparation of the food. Now fill the kettle with cold water and place over the gas and allow to boil for fifteen minutes. On a well-scrubbed worktable place a clean dish towel, and on this put the utensils and the bottles right side up. The nipples on being taken out of the boiling water will dry of themselves; they should be placed in a glass-covered jar until they are needed for each individual feeding, the nipples not being placed on the bottles as they go to the ice box.
Having been given your formula by your physician, proceed in the following way. Suppose we were preparing the food169 for a normal two-months old baby that weighed ten pounds, with the prescription as follows:
| Rx | |
| Whole Milk | ounces 11 |
| Cane Sugar | level tablespoons 2 |
| Boiled Water | ounces 12½ |
| Lime Water | ounces 1 |
| Amount at Each Feeding | ounces 3½ |
| Number of Bottles | 7 |
| Interval Between Feedings | hours 3 |
Two level tablespoons of cane sugar are placed in the agate cup and dissolved in a small amount of boiling water. The solution should be perfectly clear, and if it does not clear up put it over the heat for a few moments.
This is now turned into the eight-ounce measuring glass which is then filled with boiling water and emptied into the two-quart pitcher. We need four and one-half more ounces of boiling water to complete the prescription requirement of twelve and one-half ounces.
The bottle of milk, if properly certified, need not be pasteurized; but if it is not, it should have been previously pasteurized while the utensils were boiling according to the suggestions found in the chapter on "milk sanitation." The top of the milk bottle should be thoroughly rinsed and wiped dry, and after a thorough shaking of the milk, the cover is removed with the sterile fork and eleven ounces are measured out by measuring glass and poured into the pitcher. All is now stirred together with an ounce of lime water, which should never look murky, but should be as clear as the clearest water and should always be kept in the ice box when not in use.
The sterile cheesecloth which has been boiled for fifteen minutes is now put over the nose of the pitcher, the contents of which is accurately measured into the seven clean, empty bottles, each containing three and one-half ounces. Over the top of each of the nursing bottles is placed a generous piece of170 waxed paper which is held down by a rubber band. Each meal for the day is now contained in a separate bottle, and all are placed in a covered pail of water containing ice, and put in the ice box.
If the prescription for the baby's food contains gruel, it is prepared in the following manner:
Suppose the baby is eight months old and the prescription called for two level tablespoons of flour and eight ounces of boiled water. The two level tablespoons of flour, whether it be wheat (ordinary bread flour), or barley flour, are put into a cup and stirred up with cold water, just as you would stir up a thickening for gravy; now measure out eight ounces of water and allow it to come to a boil in the inner pan of the double boiler, into which the thin paste is stirred until it comes to a boil. After boiling for twenty minutes, remeasure in the measuring glass and what water has been lost by evaporation must be added to complete accurately the prescription requirement of eight ounces; this is now added to the other ingredients of the prescription.
We now offer a monthly schedule—a table which is the result of our experience in feeding hundreds of babies in various sections of Chicago. It is not a schedule for the sick baby, but it is a carefully tabulated outline for the normal, healthy, average child ranging from one week to one year in age. In offering this table we remind the mother, if the baby is six months old and not doing well on the food it is getting and a change is desired by both mother and physician, that it is far better to begin with the second or third month's prescription and quickly work up to the sixth month's. This change may often be accomplished in two or three days.
In all large cities there are to be found milk laboratories which make it their business to fill prescriptions for the modification of milk under the direction of baby specialists. This milk can be absolutely relied upon. In specialized diet kitchens in many large hospitals, these feeding prescriptions also may be filled.171
ARTIFICIAL FEEDING SCHEDULE
| Age | Baby's Weight | Whole Milk | Cane Sugar | Wheat Flour | Boiled water | Lime Water | Amount at Feeding | Number of Feedings | Interval Between Feedings | Fruit Juices | Soups and Broths | Total Daily Calories |
| Pounds | Ounces | Level Tablespoon | Level Tablespoon | Ounces | Ounces | Ounces | in 24 Hours | Hours | ||||
| 1 week | 7½ | 2½ | 1 | 5 | ½ | 1 | 8 | 3 | 112 | |||
| 2 weeks | 7½ | 4½ | 1½ | 9 | ½ | 2 | 7 | 3 | 184 | |||
| 3 weeks | 7¾ | 7 | 2 | 10 | ½ | 2½ | 7 | 3 | 267 | |||
| 4 weeks | 8 | 9 | 2 | 11 | 1 | 3 | 7 | 3 | 309 | |||
| 2 months | 10 | 11 | 2 | 12½ | 1 | 3½ | 7 | 3 | 351 | |||
| 3 months | 12 | 15 | 2 | ½ | 15 | 1 | 4½ | 7 | 3 | 447 | ||
| 4 months | 13 | 18 | 2½ | 1 | 13½ | 1½ | 5½ | 6 | 3 | 553 | ||
| 5 months | 14 | 21 | 2½ | 1½ | 13½ | 1½ | 6 | 6 | 3½ | 628 | ||
| 6 months | 15 | 23 | 2½ | 1½ | 10½ | 1½ | 7 | 5 | 4 | one teaspoon | one teaspoon | 680 |
| 7 months | 16 | 25 | 2 | 1½ | 8½ | 1½ | 7 | 5 | 4 | two teaspoon | ¼ cup | 732 |
| 8 months | 17 | 27 | 1½ | 2 | 8 | 1½ | 7¼ | 5 | 4 | onehalf orange | ¼ cup | 767 |
| 9 months | 18 | 29 | 1 | 2 | 8 | 2 | 7¾ | 5 | 4 | one orange | ½ cup | 854 |
| 10 months | 19 | 30 | ¾ | 2 | 8 | 2 | 8 | 5 | 4½ | one orange | ¾ cup | 875 |
| 11 months | 20 | 31 | ½ | 2 | 8 | 2 | 9 | 5 | 5 | one orange | 1 cup | 906 |
| 12 months | 21 | 32 | 7 | 2 | 9 | 5 | 5 | one orange | 1 cup arrowroot cracker | 950 | ||
| 18 months | 24 | 36 | 12 | 3 | 6 | toast, gravies, baked potato and apple, etc. | ||||||
| Note | 1 ounce of whole milk equals | 21 calories | 1 level tablespoon of flour equals | 25 calories | |
| 1 level tablespoon of cane sugar equals | 60 calories | The juice of 1 average orange equals | 75 calories | ||
| 1 level tablespoon of milk sugar equals | 45 calories | 1 cup of average bouillon equals about | 100 calories |
(This table is calculated on the basis of about 45 calories for each pound of baby weight)
Top milk is the upper layer of milk which has been removed after standing a certain number of hours in a milk bottle or any other tall vessel with straight sides. It contains most of the cream and varying amounts of milk. It may be removed by a small cream dipper which holds one ounce, or it may be taken off with a siphon, but it should never be poured off. To obtain seven per cent top milk which is the one most ordinarily used in the preparation of top milk formulas, we take off varying amounts—according to the quality of the milk—which Doctor Holt describes as follows:
From a rather poor milk, by removing the upper eleven ounces from a quart, or about one-third the bottle.
From a good average milk, by removing the upper sixteen ounces, or one-half the bottle.
From a rich Jersey milk, by removing the upper twenty-two ounces, or about two-thirds the bottle.
Cream is often spoken of as if it were the fat in milk. It is really the part of the milk which contains most of the fat and is obtained by skimming, after the milk has stood usually for twenty-four hours; this is known as "gravity cream." It is also obtained by an apparatus called a separator; this is known as "centrifugal cream," most of the cream now sold in cities being of this kind. The richness of any cream is indicated by the amount of fat it contains.
The usual gravity cream sold has from sixteen to twenty per cent fat. The cream removed from the upper part (one-fifth) of a bottle of milk has about sixteen per cent fat. The usual centrifugal cream has eighteen to twenty per cent fat. The heavy centrifugal cream has thirty-five to forty per cent fat.
The digestibility of cream depends much upon circumstances. Many serious disturbances of digestion are caused by cream.
It is convenient in calculation to make up twenty ounces of food at a time. The first step is to obtain the seven per cent milk, then to take the number of ounces that are called for in the formula desired.173
One should not make the mistake of taking from the top of the bottle only the number of ounces needed in the formula, as this may be quite a different per cent of cream and give quite a different result.
There will be required in addition, one ounce of milk sugar and one ounce of lime water in each twenty ounces. The rest of the food will be made up of boiled water.
These formulas written out would be as follows:
| I | II | III | IV | V | VI | VII | VIII | IX | |
| Oz. | Oz. | Oz. | Oz. | Oz. | Oz. | Oz. | Oz. | Oz. | |
| 7 per cent milk | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| Milk sugar | 1 | 1 | 1 | 1 | 1 | ¾ | ¾ | ¾ | ¾ |
| Lime water | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Boiled water | 17 | 16 | 15 | 14 | 13 | 12 | 11 | 10 | 9 |
| — | — | — | — | — | — | — | — | — | |
| 20 | 20 | 20 | 20 | 20 | 20 | 20 | 20 | 20 |
The approximate composition of these formulas expressed in percentages are as follows:
| Formula | Fat | Sugar | Proteins |
| I | 0.70 | 5.00 | 0.35 |
| II | 1.00 | 6.00 | 0.50 |
| III | 1.40 | 6.00 | 0.70 |
| IV | 1.75 | 6.00 | 0.87 |
| V | 2.00 | 6.00 | 1.00 |
| VI | 2.40 | 6.00 | 1.20 |
| VII | 2.80 | 6.00 | 1.40 |
| VIII | 3.10 | 6.00 | 1.55 |
| IX | 3.50 | 6.00 | 1.75 |
It is necessary to make the food weak at first because the infant's stomach is intended to digest breast milk, not cow's milk; but if we begin with a very weak cow's milk the stomach can be gradually trained to digest it. If we began with a strong milk the digestion might be seriously upset.
Usually we begin with number one on the second day; number two on the fourth day; number three at seven to ten days; but after that make the increase more slowly. A large infant with a strong digestion will bear a rather rapid increase and may be able to take number five by the time it is three or four weeks old. A child with a feeble digestion must go much174 slower and may not reach number five before it is three or four months old.
It is important with all children that the increase in the food be made very gradually. It may be best with many infants to increase the milk by only half an ounce in twenty ounces of food, instead of one ounce at a time, as indicated in the tables. Thus, from three ounces the increase would be to three and one-half ounces; from four ounces to four and one-half ounces, etc. At least two or three days should be allowed between each increase in the strength of the food.
Another modification which at times may be ordered by your physician is peptonized milk. Since it is infrequent for the proteins of milk to be the cause of indigestion, peptonized milk has only a limited use, chiefly in cases of acute illness. The milk is peptonized in the following manner:
Place the peptonizing powder (it is procurable in tubes or tablets from the drug store) in a small amount of milk, and after being well dissolved, put into the bottle or pitcher with the plain or modified milk, after which the whole is shaken up together. The bottle is then put into a large pitcher containing water heated to about 110° F. or as warm as would bear the hand comfortably, and left for ten or twenty minutes (if the milk is to be partially peptonized). To completely peptonize the milk, two hours are required. Either of these formulas is only used on the advice of a physician.
In many cases of chronic intestinal indigestion, buttermilk is used in place of the milk. It is prepared as follows: After the cream has been taken from the milk and it has been allowed to come to a boil, it is cooled to just blood heat. A buttermilk tablet, having first been dissolved in a teaspoonful of sterile water, is now stirred into the quart of warmed, skimmed milk and allowed to stand at room temperature for twenty-four hours at which time it should look like a smooth custard. With a sterile whip this is now beaten and is ready for the sugar and175 the boiled water which is added according to the written prescription from the doctor.
Under no circumstances should condensed milk be used as the sole food of the baby for more than one month. Children often gain upon it, but as a rule they have little resistance, and they are very prone to develop rickets and oftentimes scurvy; and, as noted elsewhere, orange juice should always be administered at least once during the twenty-four hours as long as condensed milk is used.
Of all the brands of condensed milk, those only should be selected which contain little or no cane sugar. Perhaps the "Peerless Brand" of evaporated milk is the most reliable and in the preparation of food from this evaporated milk the same amount of sugar, etc., should be added as we do in the preparation of "whole milk" or "top milk."
We do not in any way advise the use of condensed milk. Fresh milk should always be used where it is obtainable, but in traveling it sometimes has to be used. Holt says, "It should be diluted twelve times for an infant under one month and six to ten times for those who are older."
Malted milk is a preparation suitable in some cases where fresh cow's milk is not obtainable. Even better than condensed milk, this food will be found serviceable in traveling, or in instances where only very bad cow's milk is within reach.
Most patent foods are made up of starches and various kinds of sugars, and some of them have dried milk or dried egg albumin added. Many flours under fanciful names are sold on the market today. For instance, one flour with a very fanciful name is simply the old fashioned "flour ball" that our great, great grandmothers made; and, by the way, perhaps there is no flour for which we are more grateful in the preparation of infant food than the flour ball which is prepared as follows: A pound of flour is tied tightly in a cheesecloth and is put into a kettle of boiling water which continues to boil for five or six176 hours, at the end of which time the cheesecloth is removed and the hard ball, possibly the size of an orange, is placed on a pie pan and allowed slowly to dry out in a low temperatured oven. At the end of two or three hours, the ball, having sufficiently dried, has formed itself into a thick outer peel which is removed, while the heart which is very hard and thoroughly dry, is now grated on a clean grater, and this flour has perhaps helped more specialists to serve more sick babies than any other form of starch known. It is used just as any other flour is used—wet up into a paste, made into a gruel, which is boiled for twenty minutes before it is added to the milk.
Whey is sometimes used in the preparation of sick babies' food and is prepared as follows:
To a pint of fresh lukewarm cow's milk are added two teaspoons of essence of pepsin, liquid rennet or a junket tablet. It is stirred for a moment, then allowed to stand until firmly coagulated, which is then broken up and the whey strained off through a muslin.
The heavy proteins remain in the curd, and the protein that goes through with the whey is chiefly the lactalbumin.
A friend of ours who presides over a court of domestic relations in a large city, recently told us that he believed much trouble was caused in families—many divorces, occasioned, and many desertions provoked—because improperly fed babies were cross and irritable and so completely occupied the time of the mother, who, herself, knew nothing about mothercraft or the art of infant feeding. Consequently, the home was neglected and unhappy, quarreling abounded and failure, utter failure, resulted. The children were constantly cross, and so much of the mother's time was consumed in caring for these irritable, half-fed babies, that the home was disheveled, the meals never ready, the husband's home-coming was a dreaded occurrence, and he, endeavoring to seek rest and relaxation, usually sought for it in the poolroom or the saloon, with the usual climax which never fails to bring the time-honored results of debauch—despair and desertion.
In the beginning of this book we paid our respects to the present-day educational system which does not provide an adequate compulsory course in which all women could be given at least a working knowledge of home making and the care and feeding of the babies; so that statement need not be repeated in this chapter. But we wish to add, in passing, that ignorance is the basis and the foundation of more unhappy homes, broken promises, panicky divorces, and shattered hopes, as well as of more deaths during the first year of infancy, than any other cause. And in speaking of its relationship to babycraft, we believe that ignorance concerning normal stools, how many times a day the bowels should move; how much a baby's stomach holds; how often he should be fed, etc.—I say it is178 ignorance of these essential details that lies at the bottom of many problems which come up during the first year, particularly the "feeding problem."
In the city of Chicago at the time of this writing, the Infant Welfare Association maintains over twenty separate stations where meetings are held for mothers, where lectures are delivered on the care and feeding of babies. Babies are brought to these stations week in and week out; they are weighed and measured and, if bottle-fed, nurses are sent to the homes to teach the mother how properly to modify the milk in accordance with the physician's orders. The health authorities of our city also maintain several such stations where mothers and babies may have this efficient help. A corps of nurses are employed to carry out the instructions and to follow up the mothers and the babies in their homes, and thus the death rate has been greatly reduced, not only in our city but in all such cities where baby stations have been instituted. In a certain ward in Philadelphia the death rate was reduced forty-four per cent in one year after the baby stations were established.
There are three classes of infants who require weak-milk mixtures to begin with: namely, the baby who has been previously nursed and whose mother's milk has utterly failed; the baby just weaned; and the infant whose power to digest is low. If these children were six months old, and the formula best suited to them is unknown, we must begin with a formula suited to a two- or three-month-old child and quickly work up to the six-month formula, which may often be accomplished within two or three days.
When a baby is getting on well with his food, he should show the following characteristics: He should have a good appetite; should have no vomiting or gas; he should cry but little; and he should sleep quietly and restfully. His bowels179 should move once or twice in twenty-four hours. His stool should be a pasty homogeneous mass. He should possess a clear skin and good color. He should show some gain each week—from four to eight ounces—and he should also show mental development.
As long as a baby appears happy and gains from four to eight ounces a week and seems comfortable and well satisfied, the feeding mixture should not be changed or increased.
In our experience with the artificial feeding of infants, we have come to look upon the practice of gradually changing the food formula as the most important element in successful baby feeding.
We recall one mother in the suburbs who came to us with her baby who had been feeding on a certain proprietary food. She declared that it "just couldn't take cow's milk." She admitted "it was not doing well," and so she would like to have help. The baby was old enough, had it been normal, to have been taking whole milk for some time. We recall our having the mother prepare the proprietary food just as she had been used to preparing it, and each day we had her throw away one-half ounce and put in one-half ounce of whole milk, this mixture she fed the baby for two days.
The next time, we had her take out one ounce of the mixture and put in one ounce of whole milk, which we fed the baby for three successive days; and then one and one-half ounces were substituted which was fed to the baby for four days; and thus we carefully, slowly, and gradually withdrew the proprietary food and substituted fresh, certified cow's milk. It took us a month to complete the change, but we are glad to add that it was done without in the least disturbing the child.
Now, had the change been made abruptly—in a day or two, or three days—the baby would probably have been completely upset, while both the mother and the doctor would have been greatly discouraged. Many mothers and even some physicians have jumped from one baby food to another baby food; they have tried this and they have tried that, until the poor child,180 having been the victim of a number of such dietetic experiments, finally succumbed.
We cannot urge too strongly the fact that, as a rule, whenever a change is made from one food to another, it should be done gradually, unless it be the change of a single element such as that of a very high per cent of cream found in top milk mixtures, when it seems to be a troublesome element in the milk. No bad effects will follow the quick change to skimmed milk with added sugar, starches, etc; but in changing from a proprietary food to a milk mixture, the change should always be made gradually, the quantity of the new food being increased gradually. Milk should be increased by quarter (1/4) ounce additions, and it should not be increased more than one ounce in one week; while the mixture should not be increased as long as the baby is gaining satisfactorily. A wise mother and an experienced physician can usually see at a glance when a child is doing well—by the color and consistency of the stools, the child's appetite, his sleep, and his general disposition.
First and foremost, we believe a great mistake is often made in using too heavy cream mixtures; babies as a rule do not stand the use of too high a percentage of cream. Formulas that call for whole milk should contain four per cent fat or cream; and while babies often gain rapidly on the higher percentage of cream found in a rich Jersey milk, nevertheless, sooner or later serious disturbances of digestion usually occur. Herd milk is, therefore, better for the babies because in the "whole milk" of the herd of Holsteins we have only about four per cent fat.
Another common mistake is too heavy feeding at the time of an attack of indigestion; even the usual feeding may be too heavy during this time of indisposition. It is not at all uncommon for us to dilute baby's food to one-third its strength at the time of an acute illness.
Still another trouble maker is dirt—dirt on the dish-towel, dirt on the nipple, dirt in the milk, dirt on the mother's hands. Dirt is an ever present evil and an endless trouble maker, as181 evidenced by stool disturbances, indigestion, fretful days, and sleepless nights. A dirty refrigerator is another factor which has been responsible for much illness and distress.
Indigestion is often brought on because a nurse, caretaker, or possibly the mother, not wishing to go down to the refrigerator in the middle of the night, brings up the food early in the evening and allows it to become warm—to remain in a thermos bottle—and we are sure that had they been able to see the enormous multiplication of germs because of this warm temperature, they would never have given occasion for such an increase in bacteria just to save themselves a trifle of inconvenience.
Still another common mistake is to use one formula too long; a feeding mixture which was good for four or possibly six weeks, must be changed as the child grows older and his requirements become greater. Let the weight, stools, general disposition and sleep of the child be your guides, and with these in mind errors in feeding can be quickly detected and minor mistakes speedily rectified.
Some of the pointed questions which are put to a young mother who brings her child into the office of the baby specialist, are the following:
Does the baby seem satisfied after his feeding?
Does he suck his fist?
How much does he gain each week in weight?
Does he sleep well?
Does the baby vomit?
What do his bowel movements look like?
Will you please send a stool to the office?
With the intelligent answers to these questions—after knowing the birth weight and the age of the child and its general nervous disposition—the physician can formulate some conclusion as to the babe's general condition and can usually find a feeding formula that will make him grow.
Vomiting, restlessness, sleeplessness and the condition of the182 bowels, are the telltales which indicate whether or not the food is being assimilated; and the stools may vary all the way from hard bullet-like lumps to a green diarrhea.
Babies do not thrive well in large institutions where the food is so often made up in a wholesale manner, for the simple reason that the food elements are not suited to the need of each individual baby. Some infants are unable to digest raw milk, and for them sterilized or boiled milk should be tried; others require a fat-free mixture such as skimmed milk, while still others may need buttermilk for a short time. Babies require individual care, particularly in their food, and the good or bad results are plainly shown in the stools, weight, sleep, etc.
Flatulence is an excessive formation of gas in the stomach and bowels leading to distension of the abdomen and the belching of gas, and often the bringing up of a sour, pungent, watery fluid.
Flatulence is seen in infants suffering from intestinal indigestion and the food is nearly always at fault. This condition is the result of the faulty digestion of the sugar and starches—particularly the starch—which should be immediately reduced. In such conditions the addition of a slight amount of some alkaline (such as soda, magnesia or lime water) to the food often produces good results. Great patience must be exercised with a child that suffers from flatulence, for immediate improvement can hardly be expected; time is required for the restoration of good digestion.
Vomiting is perhaps more often the result of over feeding or too frequent feeding than anything else. A healthy, breast-fed baby may now and then regurgitate a bit, but it simply spills over because it is too full. We do not refer to this as vomiting, we refer to the belching up or vomiting of very sour or acrid milk which leaves a sour odor on the clothing. This can all usually be rectified by lengthening the intervals from two to three hours and preventing bolting of food by getting a nipple183 whose hole is not so large. Too much cream in the food will also sometimes cause vomiting.
Too frequent feeding at night is another cause of vomiting. When the stomach is full, the failure to lay the baby down quietly, as is so often seen in those homes where bouncing and jolting are practiced, may also result in vomiting.
Vomiting may be the first sign of many acute illnesses such as scarlet fever, measles, pneumonia, whooping cough, etc.
The treatment for acute vomiting is simple. All foods should be withheld—nothing but plain, sweetened water should be administered, while it is often advisable to give a dose of castor oil. A physician should be called at once if the vomiting continues, and not until the vomiting has entirely ceased for a number of hours and water is easily retained, should food be given, and even then it should be begun on very weak mixtures.
The size of the child's stomach should be the guide to the quantity of food given, and attention is called to the table given in a previous chapter. All food taken in excess of his needs lies in his stomach and intestines only to ferment and cause wind and colic. The symptoms of over-feeding are restlessness, sleeplessness, stationary weight (or loss in weight), and oftentimes these very symptoms are interpreted by the mother as sufficient evidence that the baby needs more food; and so the reader can see the terrible havoc which is soon wrought where such ignorance reigns.
The weighing time should immediately follow a bowel movement and just before a feeding time; then, and only then, we have the real weight of baby, as a retained bowel movement may often add from four to five ounces to the child's weight. There should be a careful record of each weighing, for there may develop a great difference if different members of the family endeavor to keep the weight in their minds. The normal baby should gain four to eight ounces a week up to six months,184 and from then on the weekly gain is from two to four ounces; in other words, by six months the baby should double his birth weight and at the end of a year his weight should be three times the birth weight. A stationary or diminishing weight demands careful attention; a good doctor should be called at once. Likewise, a very rapid increase in weight is not to be desired, as we do not want a fat baby, but we do desire a well-proportioned and alert baby, and, as someone has said, it is better to have little or no gain during the excessive heat than to upset the digestion by over-feeding, designed to keep the baby gaining.
In weighing, usually the outside garments are removed, leaving on a shirt, band, diaper, and stockings with the necessary pins; the little fellow thus protected is placed into the weighing basket and at each successive weighing, these same clothes or others just like them are always included in the weight, and it should be so reported to the physician.
In the chapter "Baby's Early Care," the first stools were described in detail, and there we learned that the dark, tarry, meconium stools are quickly changed within a week to the normal canary-yellow stool, having the odor of sour milk.
The bottle-fed babies' stools differ somewhat in appearance; they are thicker and a lighter color, but should always be homogeneous if the food is well digested. They do not have nearly the number of bowel movements each day that the breast-fed baby does. If a bottle-fed baby's bowels move once a day and he seems perfectly well otherwise, we are satisfied. And curds (white lumps), or mucus (sedimentary, slimy phlegm), indicate that the food is not well digested.
A bottle baby may be constipated because the proteins are too high, the fat too high, the food of an insufficient quantity or quality, or the milk have been boiled, while weak babies really may lack the muscular power to produce a bowel movement. With the help of your physician endeavor to arrive185 at the cause of the constipation, and, if the baby is two or three months old, from one to two teaspoons of unsweetened prune juice may be administered. Milk of magnesia may be added to the food (leaving out the lime water), or a gluten suppository may be used.
The change from milk sugar to malt sugar has helped many infants; while the giving of orange juice (after six months) is very beneficial in many cases. A small amount of sweet oil may be injected into the rectum which will lubricate the hard lumps and thus favor comfortable evacuation. The periodicity of the bowel movement (at definite times each day) is a matter of great importance. Immediately after a meal, if the child is old enough, he should be placed on the toilet chair. A bit of cotton, well anointed with vaseline and inserted into the rectum just before meals, will often aid in producing a bowel movement shortly after the meal has been taken.
Abdominal massage should be administered in all instances of constipation, beginning with light movements and gradually increasing, with well-oiled hands.
Diarrhoea usually accompanies acute intestinal indigestion and is so often associated with the common disorders of infancy that we refer the reader to the chapter "Common Disorders of Infancy." Dark stools should always be saved for the physician to observe, as they frequently contain blood. Stools full of air bubbles with pungent sour odor show fermentation; in which cases the starches should be reduced, if not entirely taken away from the food mixtures. Green stools mean putrefaction from filth-germs; a thorough cleansing of the bowel should be immediately followed by a reduction in the strength of the food and the boiling of the milk.
At a certain time each day the napkin should be removed and the child should be held out over a small jar. It is surprising to note how quickly and readily the little fellow cooperates. Diaper experiences may be limited to much less than186 a year if the mother has patience enough and the baby has the normal intelligence to enter into this regulation regime. We recall one caretaker who complained bitterly because the child under her care constantly wet his diaper; so the caretaker was instructed to keep a daily schedule of the baby's actions for five days; and, to her surprise, she discovered that the baby urinated about the same time each day. A regularity was also noted concerning the bowel movements.
The variations in the time of the urinations were only fifteen or twenty minutes, so nearly did the kidneys act at the same time each day. The caretaker was instructed to remove the diaper and hold the baby out at the earliest occurrence on the daily schedule, and, to the astonishment of the entire family, no further accidents occurred, and the child soon acquired the habit of letting them understand when he was about to wet his diaper. Bowel movements may be regulated more easily than the urination. After the child is about a year old, very few accidents should occur.
In many instances, and particularly if the infant is under six months of age, and where he has had to have additional feeding from the bottle—under such circumstances the breast milk may be continued as "partial feeding," at least until the baby has reached his ninth or tenth month, at which time it may be wholly discontinued.
At each nursing time the baby empties both breasts, and the amount he draws may readily be estimated by carefully weighing him before and after each nursing. By referring to the directions in a previous chapter, the quantity of food needed for his size and age may be determined; while the deficit is made up from a bottle of milk containing properly modified cow's milk.
If the mother's health admits, or if the breasts continue to secrete a partial meal for the babe, mixed feeding should be continued until after the ninth or tenth month, when it can gradually be reduced from four or five times each day to once or twice a day, until it is finally omitted altogether. In the187 meantime, the baby is gradually getting stronger food and at eleven or twelve months the little fellow is able to subsist and thrive upon whole milk.
It is very difficult to explain how some babies thrive on some certain food while others grow thin and speedily go into a decline on the same régime. The hereditary tendencies and predispositions undoubtedly have a great deal to do with such puzzling cases.
Again, sometimes a slight variation in technic or some other trifling error in connection with the preparation of the baby's food, may be more or less responsible for the variation in the results obtained. No two mothers will prepare food exactly alike even when both are following the same printed directions and these slight discrepancies are enough to upset some delicately balanced baby.
On the other hand, some babies are born with such strong digestive powers and such a powerful constitution that they are easily able to survive almost any and all blunders as regards artificial feeding, while at the same time they also manifest the ability to surmount a score of other obstacles which the combined ignorance and carelessness of their parents or caretakers unknowingly place in the pathway of early life which these little folks must tread.
The fact that so many babies do so well on such unscientific feeding only serves to demonstrate the old law of "the survival of the fittest"—they are born in the world with an enormous endowment of "survival qualities"—and in many cases the little fellows thrive and grow no matter how atrociously they are fed.
There may be other factors in the explanation of why some babies do so well on such poor care, but heredity is the chief explanation, while adaptation is the other. If the little fellows can survive for a few weeks or a few months, the human machine possesses marvelous powers of adaptation, and we find here the explanation why many a neglected baby pulls through.188
Rickets and scurvy have so often followed the prolonged use of the so-called "infant foods" which have flooded the market for the past decade, that intelligent physicians unanimously agree that they are injurious and quite unfit for continued use in the feeding of infants. If they are prescribed to replace milk during an acute illness, or at other times when the fats and proteins should be withheld for a short period, both the physician and the mother should be in the possession of definite and exact knowledge as to just what they do and do not contain. To provide such knowledge, we present the analysis (Holt) of some of the more commonly used infant foods.
1. The Milk Foods. Nestle's Food is perhaps the most widely known. The others closely resembling it in composition are the Anglo-Swiss, the Franco-Swiss, the American-Swiss, and Gerber's Food. These foods are essentially sweetened, condensed milk evaporated to dryness, with the addition of some form of flour which has been dextrinized; they all contain a large proportion of unchanged starch.
2. The Liebig or Malted Foods. Mellin's Food may be taken as a type of the class. Others which resemble it more or less closely are Liebig's, Horlick's Food, Hawley's Food, malted milk, and cereal milk. Mellin's food is composed principally (eighty per cent) of soluble carbohydrates. They are derived from malted wheat and barley flour, and are composed chiefly of a mixture of dextrins, dextrose, and maltose.
3. The Farinaceous Foods. These are Imperial Granum, Ridge's Food, Hubbell's Prepared Wheat, and Robinson's Patent Barley. The first consists of wheat flour previously prepared by baking, by which a small proportion of the starch—from one to six per cent—has been converted into sugar.
In chemical composition these four foods are very similar to each other, consisting mainly of unchanged starch which forms from seventy-five to eighty per cent of their solid constituents.
4. Miscellaneous Foods. Under this head may be mentioned Carnrick's Soluble Food and Eskay's Food.
The composition of the foods mentioned is given in the accompanying table.189
| Ingredients | Nestle's Food | Mellin's Food | Eskay's Food | Malted Milk (Horlick's) | Ridge's Food | Imperial Granum | Carnick's Food |
| Per cent | Per cent | Per cent | Per cent | Per cent | Per cent | Per cent | |
| Fat | 5.50 | 0.24 | 1.16 | 8.78 | 1.11 | 1.04 | 7.45 |
| Proteins | 14.34 | 11.50 | 5.82 | 16.35 | 11.81 | 14.00 | 10.25 |
| Cane Sugar | 25.00 | ..... | ..... | ..... | ..... | ..... | ..... |
| Dextrose | ..... | ..... | } 53.46[1] | ..... | 0.52 | 0.42 | ..... |
| Lactose (milk sugar) | 6.57 | ..... | } 49.15[2] | ..... | ..... | ..... | |
| Maltose | } 27.36 | 60.80 | ..... | ..... | ..... | ..... | |
| Dextrins | 19.20 | 14.35 | 18.80 | 1.28 | 1.38 | ..... | |
| Carbohydrates (soluble) | 58.93 | 80.00 | 67.81 | 67.95 | 1.80 | 1.80 | 27.08 |
| Starch | 15.39 | ..... | 21.21 | ..... | 76.21 | 73.54 | 37.37 |
| Inorganic Salts | 2.03 | 3.59 | 1.30 | 3.86 | 0.49 | 0.39 | 4.42 |
| Water | 3.81 | 4.73 | 2.70 | 3.06 | 8.58 | 9.23 | 3.42 |
1 Chiefly Lactose. 2 Largely Maltose.
From earliest girlhood, women have loved their dolls, and one of the greatest joys connected with the adored experience was the make-believe bath and the dressing of the make-believe baby; so now, when we are the happy possessors of real live dolls, we should go about the task with the same lightheartedness of a score of years ago when we hugged, kissed, bathed, and dressed our dolls. There is one big advantage now, the doll won't break; but, we sigh as we stop to think, we can't stick pins into it as we all did into the sawdust bodies of our dolls those years and years ago.
In the chapter on "Baby's Early Care," this subject was fully discussed and we only wish to repeat, in passing, that before baby's bath or toilet is undertaken the hands of the mother, nurse, or caretaker must be scrupulously clean. And while the first day's bath usually consists of sweet oil, albolene, or benzoated lard, if the new baby happens to come during the very warm days of July or August and the oil seems to irritate the soft downy skin, as it often does during those hot days, a simple sponge bath may be substituted. The cord dressing remains as the doctor left it, and if there be any interference, let it be subject to his orders.
The cord usually drops off, and the abdomen is entirely healed by the seventh to the tenth day, after which time baby is daily sponged for another week. And now we will describe in detail the simplest, easiest manner of administering an oil bath or a sponge bath.191
A large pillow or a folded soft comfort is placed on a table in a warm room—temperature not below 75 F. On baby's tray near by, and within reaching distance, are the boracic acid solution in a small cup, a medicine dropper, the warm saucer of oil, the toothpick applicators (made by twisting cotton about one end, making sure the sharp end of the pick is well protected), a glass jar of small cotton balls made from sterile absorbent cotton, the castile soap, talcum powder, needle and thread. A vessel of warm water, several old, soft, warmed towels and the clean garments required, complete the layout.
Into the warm, soft blanket on the pillow or comfort we place the partially undressed baby, for the binder, diaper, and socks are not removed until the head-and-face toilet is completed.
The top of the head, behind the ears, the folds of the neck, and the armpits are now gently but thoroughly rubbed with oil, which is then all rubbed off with a soft linen towel. The eyes next receive two or three drops of the boracic acid solution, put in by the aid of the medicine dropper, while, with a separate piece of cotton, the surplus solution is wiped off each eye, rubbing from the nose outward.
Then with the applicator made by wrapping cotton about the end of a toothpick, oil is put into each nostril, all the time exercising the utmost care not to harm the tender mucous membrane. The ears are also carefully cleansed with a squeezed-out dip of boracic acid on the applicator.
Unless there is an inflammation present in the mouth, and the physician in attendance has ordered mouth swabbing, do not touch it; for much harm is done the mucous membrane of the baby's mouth by the forceful manner in which much of the swabbing is done. The face and head are then washed with warm water; very little soap is needed and, when used, must be most thoroughly rinsed off.
And now during the second week, we proceed to sponge the baby's body; the hands are washed with soap and rinsed, and,192 only those who have performed this feat know just how tightly they hold shut their little fists. These hands must be relaxed, and all the lint, dirt, and perspiration be thoroughly washed away. The arms, shoulders, chest, and back are then sponged. All the time the nurse or caretaker is standing while carrying out this most pleasant task. At any time she may quickly cover the babe and stop for this or that with no inconvenience to herself or the child.
After the thorough drying of baby's upper body, a bit of talcum is put under the arms, in the folds of neck, etc., and the shirt is slipped on. Next the band, diaper, and stockings are removed and after first oiling the groin and the folds of the thighs and the buttocks, the same sponging, drying, and powdering is done here as on the upper body.
The band is now applied, and sewed on. The diaper, stockings, booties, and—if a winter baby—the skirt and outing flannel gown (for babies should wear only night dresses for the first two or three weeks) are now slipped over the feet and drawn upward, and baby is ready for nursing or for his nap.
First few weeks, 100 F.; early infancy, 98 F.; after six months, 97 F., cooling down to 90 F.
A wooden bath thermometer may be purchased for twenty-five cents and it should be in every home where babies are bathed. In the absence of a thermometer do not depend upon the hand to determine temperature. Thrust the bared elbow into the water and if it is just comfortable—neither hot or cool—it is probably about the correct temperature for baby. Do not shock the baby by dashes of cold water, for, while it may amuse an onlooker, it unnecessarily frightens your child, and, subconsciously, he learns to dread his bath.
If the bathroom is warm—temperature 75 F.—that is the most logical place for the bath, provided baby has his own tub. Place a couple of strong slats several inches wide across the big tub, six inches apart, and on this place the baby's tub. Of193 course, care must be exercised to prevent slipping by means of properly fitted cleats on the under surface of the slats. The mother should always stand to bathe her baby and the small tub should be placed at such a height that she neither has to stoop nor bend. Thus the bathing of the baby becomes a pleasure instead of a "job" or an "irksome task."
If the bathroom is not warm then the kitchen table or a small table pulled up near the stove is a place par excellence for the dip.
Many boils seen on young baby's tender skin have been traced to the careless use of the family tub to bathe the baby in. Not until the child is two or three years of age, when his skin has become more toughened, should he be allowed to use the family tub.
To begin with, we never bathe either a baby or an adult immediately after a full meal. From one hour to one and one half hours should intervene.
The frequency of baths depends somewhat upon the season of the year, the vitality of the child, and the warmth of the home.
We have seen many infants who were bathed too often. The vitality expended upon the necessary reaction following a tub bath was too much for the little fellow; the daily bath was stopped and a semi-weekly bath substituted, much to the gain of the child. Of course in this instance the hands, face, and buttocks received a daily sponging.
The oil bath may be administered daily. In robust children the tub bath may be a daily affair; while in pale, anemic little folks, the tub bath is perhaps better given twice a week. In hot summer days a sponge bath may be given many times a day.
Again this depends upon several factors; the warmth of the house or apartment, the vitality of the child, and the kind of bath to be administered.194
An oil bath may be given any time—often it may be administered entirely under the bed clothes, only care must be taken to keep oil from the blankets.
Many of our mothers prefer to give the tub bath at five o'clock in the afternoon, when the house is thoroughly warm, and the child is thereby prepared for the long night's sleep. Before dressing in the morning an oil bath or rub may be given in such cases.
If the forenoon is selected as the time for bathing the child, then an hour just before the mid forenoon meal is the best. In either event, be regular about it—do it at the same time every day. Let the caretaker attend to her many duties, and, as far as possible, mothers, bathe your baby yourself. The folds of the skin, the creases in the neck, the clenched fists, must all receive particular care, and no one in all the world will ever care as you—the mother—cares.
Select a soap free from irritants and excess of alkalis. There are few kinds that equal the old-fashioned, white castile soap our grandmothers used.
Very hard water which makes the skin rough and sore may be improved by boiling, but if possible substitute rain water for it. A flannel bag tied over the faucet and changed each day will help to clarify muddy water, provided the stream flows gently through it.
Just as we directed the nurse or caretaker to stand while the oil rub or sponge bath was given, so we admonish the mother to stand while the tub bath is given. First, get everything in readiness for the bath as directed for the oil bath, and then the baby's tub setting on the securely cleated slats placed across the top of the family tub may be filled with water by means of a hose attached to the faucet. The temperature should be 100 F. when baby is dipped in to be rinsed.
The head and face toilet are identical with that described before, and with the baby undressed and wrapped in a warm 195towel placed inside the warm blanket on the pillow or comfort as before mentioned, we proceed with a good lather of castile soap and water to lather the baby's body all over—under the arms, the neck, chest, groins, thighs, buttocks, legs, feet, and between the toes, while the genitals also receive their share of attention. The foreskin of the boy baby is gently pushed back and cleansed thoroughly; while the vulva of the little girl baby, having first been swabbed with boracic acid, is now gently lathered and cleansed. Now grasp the ankles and legs with the right hand and support the upper back and neck and shoulders with the left and gently lower the baby into the water in a semi-reclining position (See Fig. 13). The water should cover the shoulders. Keep a good firm supporting left hand under the head, neck, and shoulders, and with the right, rinse all soap from the body.
After this is thoroughly done, lift the baby out onto a fresh warm towel inside the warm blanket on the pillow, and remain standing, while you gently pat (never rub) the baby dry. All the little folds, creases, and places between fingers and toes, are carefully patted dry, and where any two skin surfaces rub together put on a bit of talcum.
The dressing takes place in the manner already described—first the shirt, then the band (sewed on), the diaper, stockings, skirt, and gown.
Please note that the soap bath is contra-indicated (should not be given) in case of eczema.
This soap bath should be administered for cleanliness only, and should be given twice a week. If a tub bath is to be given on other days, after the routine head and face toilet, the baby is simply dipped into the water and the soft skin gently rubbed.
If the sponge or tub bath is given in the afternoon just before the long sleep at night, then the oil rub should take place before the mid-forenoon meal; and likewise, if the sponge or tub bath is given during the mid forenoon, then the oil rub or dry hand rub is given before the going-to-bed time. The rub should be a daily procedure for the first two years. Nothing196 rougher than the soft palm of the hand should be rubbed on baby's soft skin.
Babies have come to my clinic with cakes of talcum under their arms, and particularly between their thighs and in the crease of the buttocks. Here the well-meaning but thoughtless mother had reasoned, "a little is good; more is better" which is not always the case.
Talcum is not used to replace careful drying, and it should never be found in quantities on the baby's skin any more than you would expect to find quantities of face powder caked in the creases of the neck or behind the ears of an adult. The skin is first cleaned, then patted entirely dry, and, as a finishing touch, a bit of talcum is put on by means of a puff.
Tonic baths are usually given to older children when they are able to enter into the sport and frolic of a cool bath. Baths are called tonic because they call forth from the body a reaction—a sort of circulatory rebound. This rebound or reaction brings the blood to the skin, increases the circulation, and tones up the nerves. The room should be properly warmed and, if necessary, some form of exercise be continued after the bath to prevent the chill that sometimes follows a poorly administered bath.
In the case of the anemic child, after six months of age, the mother's hand dipped in cold water may briskly rub the chest and back until it glows or becomes red. The child should enjoy this bath. Never frighten a child by throwing cold water on it or by giving it a too sudden cold plunge; great harm may be permanently done by these efforts to "toughen the baby."
The simple medicated baths may be administered according to the following directions:
Salt. Use half a teacup of common salt or sea salt to each gallon of water. The salt should first be dissolved in a cup of warm water to prevent the sharp particles from pricking the skin. The doctor sometimes orders a salt bath.197
Starch. Add a cup of ordinary, cooked laundry starch for every gallon of water in the bath.
Soda. A soda bath requires two tablespoons of ordinary baking soda to a gallon of water, dissolving it in a little water before adding it to the bath.
Bran. Make a cotton bag of cheesecloth or other thin material, six inches square. Fill loosely with bran. Soak the bag in the bath water, squeezing it frequently until the water becomes milky.
Starch, soda, and bran baths are often used in place of the ordinary soap and water bath when the skin is inflamed, as in cases of chafing or prickly heat.
Force and harshness are not likely to cause baby to overcome very much of the fear of a tub bath. Patience, perseverance, and purposeful diversion of mind will bring sure results.
In the case of a very young baby, have a helper stretch a towel across the filled baby tub, lay the baby in it, with its head well supported, and then gently lower the towel into the water, keeping the head out. (Most anyone would fear an all-over ducking, if he had ever been completely ducked into water by a careless or mischievous friend).
In the case of older children, celluloid ducks, fish, or boats may float about on the water, and the entire bath be forgotten by the little fellow's enjoyment of "his boats."
Although a baby under two years should never be given a sea bath, a word of caution about sea bathing for young children may not be amiss. The cruelty with which well-meaning parents treat young, tender children by forcibly dragging them into the surf, a practice which may be seen at any seaside resort in the summer, can have no justification. The fright and shock that a sensitive child is thus subjected to is more than sufficient to undo any conceivable good resulting from the plunge. On the other hand, a child who is allowed to play on the warm sand and becomes accustomed to the water slowly and naturally will soon learn to take delight in the buffeting of the smaller waves, but he should198 not be permitted to remain more than a minute or two in the water, and should be thoroughly dried, dressed immediately, and not left to run about the beach in wet clothing.
Any roughness on the scalp must receive immediate attention. This roughness, or milk crust, is entirely avoidable; it is the result of accumulated oil and dirt. When it has formed a complete crust or cake, it may quickly become eczematous and require a physician's advice; however, in the beginning, at the first sight of brown patches or roughness, oil the scalp thoroughly at night with vaseline or cold cream, which should be gently rubbed off in the morning.
This vaseline or cold cream should be applied repeatedly, several nights in succession, followed by the morning's gentle rubbing and daily washing of the head. Often the washing with water must be entirely avoided; only sweet oil or vaseline being used in those cases where the crusting seems to be persistent.
At birth the eyes are particularly cared for. First, the mucus is gently swabbed off the closed lids from the nose side outward, and then follows the application of one drop of twenty per cent argyrol or two per cent silver nitrate, either of which thoroughly disinfects the eye and prevents the growth or development of any bacteria that may have gotten into the child's eye during the descent of the head through the birth canal. The neglect of this procedure may sometimes result in lifelong blindness.
Under no circumstances should "a mere cold in the eyes" be neglected; it may result in blindness. Call your physician at once, and if he is not at hand, wash out the eye thoroughly every hour with warmed ten per cent boracic acid solution, by means of a medicine dropper, using a separate piece of cotton for each eye, for if the slightest bit of discharge be carried from one eye to the other an inflammation will quickly appear.
From birth, especially during the first week, baby's eyes are199 very sensitive to light; hence they must be carefully protected. Babies should be so placed during their outings, sleep, or naps, that they do not directly gaze at either the sunlight or sky. The lining of the hood of the carriage should be green, instead of white, as much eye strain is thus prevented.
The daily care of the normal, well eye has been already described, and while it need not be reiterated, we may say, in passing, that if the eyelid be at all inclined to be sticky or adherent, never use force, but instead, gently swab with boracic acid. As a preventive of this condition, a little vaseline from the tube may be rubbed on the edges of the lids at night.
In the toilet of the ears, never attempt to introduce anything beyond the external ear, which may be carefully cleansed with a soft cloth. It is often found necessary to apply oil to the creases behind the ears before the daily bath. There should be no irritation, redness, or roughness present, all such conditions being readily prevented by the use of oil or vaseline before the bath.
With the sharp point removed, make a cotton applicator out of a toothpick, and gently (with no force, whatever) introduce vaseline or oil into the nose. This should be a part of baby's daily toilet. Any stoppage of mucus or snuffiness in the nose should be reported at once to baby's physician. Young babies often have adenoids.
Leave the well mouth alone until the teeth appear, and then keep the teeth very clean (allowing no particles of milk to accumulate at their bases) with a soft bit of cotton and gentle rubbing. When a child attains the age of two, he should have his own toothbrush; previous to this time all food particles should be removed from between the teeth with waxed silk floss. All decay should be promptly attended to by a competent dentist.
Thrush and ulcers are often caused, not prevented, by the frequent wiping out of baby's tender mouth. The treatment of thrush and other mouth infections will be considered in a later chapter, "The Common Disorders of Infancy."200
Before the bath, the baby girl's genitals are carefully swabbed between all the folds with boracic acid solution. The foreskin of the boy baby should be pushed well back and washed gently with water. If the foreskin of the male child be long, tight, or adherent, circumcision is advised. See our chapter, "Teaching Truth."
The genitals of both the boy and girl should be kept scrupulously clean every day, with as little handling as possible, and, upon the appearance of the least swelling, discharge, or even redness, the physician's attention should be at once called to it. In a later chapter, the subject of irregularities of sex habits will be taken up.
Often, because of irritating bowel movements, the buttocks become reddened, chafed, and sometimes raw in places. Some poor little babies are sometimes roughly rubbed—scoured on the buttocks—much like the kitchen sink, many times a day, and it is not surprising that they become reddened, chafed, and very much inflamed.
The buttocks require a gentle swabbing and thoroughgoing "patting dry" after each soiling or wetting of the diaper, but no soap is required in this region but once a day, and even then it should be used sparingly.
When the buttocks are inflamed, after a good cleansing with water and a thorough drying, vaseline or zinc ointment should be applied on a piece of sterile cotton, and this application should be repeated after each changing of the diaper. Wet diapers should be removed at once, for the acidity of the urine causes more chafing. A dusting powder composed of starch two parts, and boracic acid one part, may be dusted on after a cleansing with oil.
Great care should be exercised in the thorough daily rinsing of the diapers as well as in the tri-weekly boil in the laundry. White soap only should be used in their cleansings; no washing sodas or other powders should be used.201
Under the arms and in the creases of the neck the skin sometimes becomes irritated because of neglect. To prevent such chafing the following program should be carefully carried out:
With a fine camel's hair brush the hair should receive its brushing after the cleansing of the scalp. Combs are for just one purpose and that is to part the hair. The brush should be used to do all the smoothing.
While the frequent trimming of the hair has no marked effect upon its growth, yet the comfort the little girls enjoy, especially during the warm-weather months, should not be denied them.
And certainly the boy should become a boy when he puts on trousers and not be made the laughing stock of his mirthful companions just because his "beautiful long curls are much admired by the mother and his aunts."
The finger nails should be trimmed round with the scissors, while all hangnails are properly cared for every day. Toe nails should be cut straight across and the corners never rounded off. Many ingrowing nails may be thus avoided.
The Eden story suggests that in the beginning of our racial experience artificial clothing was unnecessary; but after a time, in that selfsame garden, proper clothing became an important problem and has remained so ever since. Everybody seems to agree, however, that baby's clothing in particular should at least be comfortable. It may give the child great discomfort because it may be too warm, or it may not be warm enough, or it may be too tight, and so, in the discussion of baby's clothing in this chapter, we are going to keep in mind these two things—comfort and heat.
The choice of material demands some thought and attention. As a rule, baby's clothing materials should be light in weight, good moisture absorbers, and at the same time able to retain the body heat. Most layettes have the common fault of being prematurely outgrown; and so it is well to allow for ample growth in making baby's first clothes. Since the principal object of clothing is to insure a uniform body temperature, it is important that the mother be constantly on her guard to keep the baby cool enough in the summer and warm enough in the winter.
The mothers of various races and nations have their own ideas concerning the clothing of their babies. One mother will wrap her baby in cotton, which is held in place by means of a roller bandage, and as you visit this home during the first week of baby's life, you will be handed a little mummy-shaped creature—straight as a little poker—all wrapped up in cotton and a roller bandage. The surprising feature is that the baby does not seem to complain.203
In another district of the city we find the baby dressed in starched clothes, ribbon sashes, bright ribbon bows on its arms and around its neck. At first glance you wonder if the little child is not many years older and is about to make a visit to a county fair, but on inquiry we find that he has only been prepared for the event of circumcision on the eighth day.
And if you go into the forest of primeval days you will find another mother bandaging her baby to a board, head and all, and he seems to live and thrive in his little woven nest strapped on the back of his Indian mother.
Other babies in the warmer portions of the earth have almost less than nothing on, and are left to be swung by the breezes in little baskets tied to the boughs of trees; being taken up only when it is time to feed.
In preparing an outfit for the newcomer it is wise to provide for the necessities only, because of the fact that since the baby grows very fast the layette will soon have to be discarded; it is always possible to get more clothing after the baby is here and started on his little career. We offer the following list of essentials for the new born baby:
| Slips | 8 to 10 |
| Skirts (flannel) | 3 |
| Shirts | 3 |
| Light-weight wool wrappers | 2 |
| Abdominal bands | 3 to 5 |
| Diapers (first size) | 2 doz. |
| Diapers (first size) | 2 doz. |
| Stockings, pairs | 3 |
| Booties, pairs | 3 |
| Nightgowns | 7 |
| Handling blankets | 2 |
| Silkaline puffs | 2 |
| Baby blankets, pair | 1 |
| Hair or cotton mattress | 1 |
| Basinet | 1 |
The binder should be made of an unhemmed strip of flannel six inches wide and twenty inches long, so that it goes around the abdomen once with a small overlap. This binder should be sewed on instead of being pinned, and serves the purpose of holding the dressings of the cord in place. It is usually worn from four to six weeks, when it is replaced by a silk and wool barrel-shaped band with shoulder straps and tabs at the bottom, both front and back, to which may be pinned the diaper. This band is worn through the first three or four years to protect the abdomen from drafts and chilling, thus guarding against those intestinal disturbances which are caused by sudden weather changes.
There is great danger of having the bellyband too tight, and, in the early weeks, it is often the cause of great discomfort—often interfering with the normal expansion of the stomach at meal time.
No matter what the season, the new-born baby should be clothed in a light-weight silk and wool shirt, preferably the second size. After the first month, if the weather is exceedingly warm, this woolen shirt may be displaced by a thin silk or lisle shirt. In buying the second-size shirts always secure the stretchers at the same time, for in the laundering they soon shrink so that they are very uncomfortable for the young babe.
There are a number of materials on the market from which comfortable diapers may be made for the baby. The cotton stockinet (ready-made shaped diaper) is excellent, fitting smoothly at the waist, while it is large and baggy at the seat, thus permitting not only a comfortable feeling but the free use of the hips, without the bulkiness of the ordinary diaper.
The large square of cheesecloth is easily laundered, and if an inside pad is used makes a very acceptable diaper.
The stork diapers are made of materials resembling turkish toweling and are used to some extent. This diaper should not be confused with the stork rubber diaper which will be spoken of later.205
Birdseye cotton is popular and extensively used. It absorbs quickly, and is much lighter in weight than linen. The first- and third-size widths should be purchased as a part of the layette, and the number of diapers needed depends upon the opportunities to wash them out, for diapers are never used but once without washing; they should always be quickly rinsed and dried in the sunshine if possible. So if there are good laundry privileges, and daily washing is possible, the mother can get along with fewer diapers, but no less than four dozen should be provided.
The diaper pad will be found convenient and serviceable in the early days when the skin of the child is so very tender. This pad should be pieces of clean old linen or small pads of absorbent cotton.
During the mother's waking hours, the diaper should be changed as soon as it is soiled or wet. If the child cries during the night it should be changed immediately, but the mother should not feel called upon to lay awake nights merely to change the baby's napkin when it is soiled. If she places a pad underneath the baby, which will absorb the urine quickly, he often does not awaken or become chilled. The pad should be sufficiently thick to ensure that the nightgown does not get wet.
Rubber sheeting diapers of any description should never be used. Avoid all patent diapers with a covering or an inner lining of rubber, for, like the rubber diaper, they not only irritate the child but also retain moisture and heat, which produce such irritation and itching that the subsequent "habit-scratching" often lays the foundation for future bad practices. It is far better for the mother to carry about with her, whenever it is necessary to take the baby away from home, a rubber pad which she puts on her lap underneath the little fellow, thus affording ample protection to herself without in the least harming the baby.206
During the winter months merino stockings are required, while during the summer months a thin wool or silk stocking is sufficient; on the extremely hot days thin cotton hose may be worn. During infancy, the stockings should be fastened to the diaper with safety pins, while on the second-year child, hose supporters attached to the waist are found very convenient.
A friend told me the other day of a mother who told her the following story: "Do you know, I don't have any trouble any more about my baby keeping up his socks for I have fixed it so they won't come off any more. Every time I looked at his feet he had kicked off his socks and they were no good to him at all, so I took little chunks of brown laundry soap, moistened them and rubbed his legs, as well as the inside of his socks and I never, never have any more trouble with them coming off."
It does not seem possible in this enlightened age that a mother could be so ignorant as to keep the socks up with brown soap, but the friend assured me it was a true story, and while it may shock some of my readers as it did me, I must add, in passing to another subject, that the use of round garters on little babies and young children is just about as shocking.
During the fall, winter, and spring, booties are worn on top of the stockings. These booties should be crocheted or knitted out of the heavy Germantown yarn, and there should be enough of them so that the child may have a clean pair on every day.
The flannel petticoat is made with yokes instead of bands, and during the fall, winter, and spring these yokes are made of flannel like the skirt and should have long sleeves of the same material. The yokes should be made large enough so that they may be used during the entire first year (the plait in the front can easily be taken out when the baby is six months old so that it may be used much longer than if the yoke is made without a plait). For the hot summer months, the yokes should be a thin cotton material without sleeves; and, if the baby is housed in an over-heated apartment, this fact should be borne in mind and the winter skirt should be made accordingly. We have207 found, however, that the baby who is amply protected and uniformly dressed, does not require the outer bundlings that the poorly dressed child requires. Part wool and cotton materials are very comfortable in the overheated city apartments. White skirts are not necessary for small babies. They only add extra weight and it is always foolish to put anything on a small baby simply for looks.
The nightgowns should be made of soft cotton flannel or stockinet. The latter is really the better, and can be purchased in sizes up to two years; it is absorbent, easily laundered, and may be conveniently drawn up at the bottom by means of a drawstring.
At least seven nightgowns are needed. A fresh nightgown should be used each day and each night during the first four or five weeks of baby's life; while as he gets older (two or three years), the night drawers with feet in them are used to advantage.
The wrappers are usually made of challis, nun's veiling, cashmere, or other light woolen materials which can be readily washed. They are very serviceable to wear over the baby's thin slips and on cool nights they may be used over the nightdress. They should be simply made, containing no heavy seams, and at the neck there should be the simplest kind of a soft band that will in no way produce friction or in any other way irritate the baby's skin.
Slips are usually made of some very soft material such as nainsook, batiste, pearline, or sheer lawn cloth. Twenty-seven inches is the length that will be found both comfortable and convenient. All laces, ruffles, and heavy bands which will scratch or irritate should be avoided as eczema is often caused by such mistakes.
The sleeping bag is of inestimable value, affording extra and secure covering for the child, and peace of mind for the mother. In the early weeks it should be made of light flan208nel, but as the child gets older the sleeping blanket is made according to illustration (See Fig. 7) by merely folding a blanket in such a manner that the child cannot possibly uncover himself. The mother can sleep undisturbed, knowing that the baby is always safely protected by at least one warm blanket cover.
As a usual thing the first clothes are made too small. The sleeves are too short as well as too small around. There is nothing more uncomfortable than a tight sleeve. Everyone of our readers knows that, and we recall one poor little fellow who kept up a fretful cry until we took the scissors and cut the tightly stretched sleeve up to and including the arm hole. He then relaxed and went to sleep. Sleeves should be made two inches longer than they are needed at first, and it is a very simple matter to pin them up or turn them back at the wrist. They should be loose and roomy.
The yokes of the dresses usually are too tight before the slips are discarded. Heavy seams and raw seams irritate and often make ugly impressions on the baby's skin.
Usually the first layette is profusely embroidered, and, while it is beautiful to look at, the mother feels when she sees it outgrown so quickly that a lot of vital energy was wasted on garments that mattered so little as long as baby was comfortable. Baby is dear and sweet enough without the fuss and furbelows of such elaborate garments.
Heavy materials are sometimes used where lighter ones would serve better.
A soiled garment should never be put back on the baby. Dirt draws flies, and flies are breeders of disease. Sour-smelling garments should be changed at once. They are likely to make the baby sick and interfere with his appetite if left on indefinitely. The care of the diaper has already been mentioned.
The main symptom of too much clothing is sweating, and when the baby sweats something must come off. If he has209 perspired so much that his clothes are moist, the clothing should be changed and the skin well dried with talcum powder. The feet and hands should be kept warm, but the little head should always be kept cool. When the baby is crying and getting his daily exercise, remove some of the covering, loosen his diaper, and let him kick and wave his arms in perfect freedom.
When the baby's feet and hands are cool he is not warm enough. Cotton underskirts cannot be used in the dead of winter on little babies. They do not hold the body heat as woolen garments do. The baby's feet should always be warm and this is particularly necessary in poorly nourished children. The outer wrapper of woolen material should be added to such baby's clothing. It is a safe rule to follow that if baby's hands are warm and he is not sweating, he is "just about right."
At the age from four to six months, baby's clothes are shortened. This should not take place at the beginning of winter if it can be avoided. If the first layette has consisted of only the necessary garments, they are nearly worn out by the time the short clothes are due; of those that do remain, the sleeves should be lengthened, the arm holes enlarged, and all the little waists let out. Creeping garments and bibs are now added to baby's outfit, as well as leggings and other necessities for outdoor wear. Remember that all garments must be loose—then baby is happy.
About the same number of garments are found necessary for the short clothes as were required at first; except that a large number of creeping rompers should be added. These creeping rompers should not be made of dark materials that do not show the soil. We desire the dirt to be seen that we may keep the baby clean, and if the creeping romper is made of a firm, white material it may be boiled in the laundry, thus affording ample and thorough cleansing.
We attributed a sick spell of one baby to the dark-blue calico creeping romper which he wore day in and day out because it "did not show" the soil. White ones are much to be preferred, not only for looks but chiefly for sanitary reasons.210
The cap should be made of a material that will protect from drafts and cold air, but not of such heavy materials as will cause too much sweating. There are a number of outside wraps that can be purchased ready-made and which are comfortable, convenient, and warm. They should be long enough not only to cover the baby's feet well, but to pin up over the feet, thus giving good protection from winds and drafts.
During the summer months nainsook caps or other thin materials are to be preferred to the heavy crocheted caps that are sometimes worn by babies. No starch should be used in the caps or strings, and there should be no ruffles to scratch the delicate skin of the baby. In all these outer garments, as well as the under garments, the irritation of the skin must be constantly borne in mind, as eczema is often produced in this manner.
The first shoe that is usually worn during the creeping days is a soft kid shoe without hard soles. It is important that this soft shoe be worn to protect the child's foot from chilling drafts while creeping about.
As the baby nears one year of age the hard-sole shoe is secured which must be wide, plenty long and comfortable in every respect, and without heels. Rubbers and overshoes may be worn on damp and cold days. Moccasins and slippers do not give sufficient support to the ankles, so, when the baby begins to walk, the shoes should be high and of sufficient support to the tender ankles.
As the baby grows up into the child, the tiny clothes are laid aside and the boy is given substantial garments that in no way remind him of girls' clothing. A child's feelings should be respected in this manner, and while it often adds joy to the mother's heart to see her boy "a baby still," remember that he is not only chagrined but is nervously upset by these "sissy clothes."211
A child three or four years of age should still wear the woolen binder supported from the shoulders, over which is the union suit, stockings, and the buttoned waist from which hang the hose supporters. The most comfortable and easily laundered garment we know of for the small lad is the "romper," which should be made of washable materials that may be readily boiled. For cool days a Buster Brown coat of the same material, with patent-leather belt, may be slipped on over this washable romper—which completes the boyish outfit.
We recall the pleasant days with our own little fellow when he was between the ages of two and one-half and five years. We were often compelled to be away from home—on the train, in the hotel—and when traveling we used a black, smooth silk material which was made up into rompers with low neck and short sleeves. There were three such rompers, and two Buster Brown coats with wide, black, patent-leather belts which completed the traveling outfit. During the warm days on the train the coat was folded carefully and laid aside. In the early morning and in the cool of the evening the coat was put on, and he always looked neat and clean. At night, before undressing him, the entire front of the romper was cleansed with a soapy washcloth, rinsed, and rubbed dry with a towel, and, after carefully spreading to avoid wrinkles, it was hung over the foot of the bed. The coats were sponged or pressed once or twice a week, and this simple outfit served its purpose so well that it was repeated three different summers.
The little girl as she leaves her babyhood days should be put into garments that do not necessitate the constant admonition, "Keep your dress down, dear." We like to see knickerbockers, the exact color of the dress, made for every outfit, in which the little girl may kick, lie down, jump, dance, climb—do anything she pleases—unmindful of the fact that her "dress is not down." The same undergarments are used for the little girl as were mentioned for the little boy.
Always bear in mind the over-heating of the child with heavy garments indoors, and the danger of skin chilling and drafts on212 going out to play in this over-heated condition. Let the children dress comfortably cool in the house, and as they go out to play add rubber boots or leggings and rubbers, sweaters, caps with ear laps or the stockinet cap. Allow them the utmost freedom in clothes, and always encourage romping in the cool frosty air.
Do not overload the baby with clothing.
Dress according to the temperature of the day and not the season of the year.
Avoid starched garments.
Avoid tight bellybands or old-fashioned pinning blankets.
Change all clothes night and morning.
Use woolen shirts and bands.
See that hands and feet are always warm.
Protect the abdomen night and day with the band.
Use the sleeping bag on cold nights.
Baby should sleep in loose stockings at night.
Avoid chilling the child.
Use hot water bags if necessary.
Fresh air is just as important and necessary for the baby as for the adult. Neither baby, youth, nor adult can receive the full benefit of his food—in fact it can not be burned up without the oxygen—without an abundance of fresh air. During the early weeks of life, the air baby breathes must be warm; nevertheless, it must be warmed fresh air, for baby requires fresh air just as much as he needs pure food.
The delicate child often requires more fresh air than does the normal baby. Both appetite and sleep are improved by fresh air. The digestion is better, the cheeks become pink, and all the signs of health are seen in the child who is privileged to breathe fresh air.
During the early days, say after the third week, baby should be well wrapped up with blanket and hood, tucked snugly in his basinet or carriage, while the windows are opened wide and the little fellow is permitted to enjoy a good airing. Even in the winter months the windows may be raised in this way for a few minutes each day. These "airings" may be for ten minutes at first, and, as the child grows older, they may be gradually increased to four or five hours daily. The carriage or basket should stand near the window, but not in a direct draft.
In summer, a baby one week old may be taken out of doors for a few minutes each day; in the spring and fall, when baby is one month old, it may go out for an airing; while, during the winter months, the airing had better be taken indoors until214 he is about two months old, and even at that age he should go out only on pleasant days and should always be well protected from the wind.
A young baby may enjoy the fresh air in his carriage or crib on the porch, on the roof under suitable awnings, in the yard, under the trees, and even on the fire escape. In fact, at proper age and in season, he may spend most of his time out of doors in the fresh air, if he has proper protection from the sun, wind, and insects.
During the balmy days of summer and early autumn, baby may spend most of the time outdoors between seven in the morning and sunset. During the cooler days of winter and the cool and windy days of spring, the best hours for the airing are to be found between eleven in the morning and three in the afternoon.
At six weeks, perhaps an hour a day in the fresh air is sufficient; while at six months, four to six hours a day are a necessity, and from then on—the more the better.
Now we realize that the mother of the farm household does not always have as much time to take the baby out for his airings as many of our city mothers; but we suggest to this busy mother that the baby be rolled out on the porch or in the yard, within her sight and hearing, and allowed to enjoy the fresh air while the mother continues her work.
It is virtually a crime to try to keep baby in the kitchen, hour after hour, while the busy mother is engaged at her tasks. A hammock, a crib on casters, or a carriage, is just the coziest place in the world for baby—out on the porch.
The average city baby really gets more fresh air than ninety per cent of the country babies. Our city apartments are usually steam heated, and our windows are open in the winter nearly as much as in the summer. The country home is often only partially heated by two or three stoves. The windows are closed in summer to keep out the dust, heat, and flies, in the winter to215 shut out the cold, and so the baby who lives in such a home has little chance to get fresh air.
The city mother is constantly talked to about the benefits of fresh air. The daily paper brings its health column to her, her pastor talks of it on Sunday, and—best of all—the older children come home from school and reiterate the doctrine of fresh air that is constantly being preached to them at school.
Screen the windows, rural mother, and oil the roads in front of your residence, and then keep your windows open. Remember that baby's health is of more value than the meadow lot or even a fortune later on in life. Plan for a new heating plant, if necessary, so that the home can be both warmed and ventilated during the winter.
If a sheltered corner of the porch is within the reach of the mother, we can hardly think of a time when the baby cannot be taken out. It may rain, the wind may blow, it may snow or even hail, but baby lies in his snug little bed with a hot water bottle or a warmed soapstone at his feet. As long as the finger tips are warm, we may know he is warm all over, and a long nap is thus enjoyed in the cool fresh air. When the sheltered corner of the porch is lacking, we wish to caution the mother concerning the following weather conditions:
1. When the weather is excessively hot, take him out only in the early morning and late in the afternoon.
2. In extremely cold, below zero, weather, let his airing be indoors.
3. Sharp and cold winds may do much mischief to baby's ears, as well as blow much mischief-making dust into his nose and eyes. In the case of dust or sand storms, baby remains in the house.
4. All little people enjoy the rain, and only when the raincoat, rubbers, and umbrella are missing should they be robbed of the "rainy-day fun". In the case of baby's outing on rainy days, ample roof protection is the only factor to be considered; if it is adequate, then take him out; if it is lacking, let the airing be done indoors.216
The very young baby is taken out for a fifteen-minute airing during the noon hour when he is two months old; before this time he receives his airing indoors. The interval is gradually lengthened until most of the time between eleven and three is spent out of doors. The reddened cheeks, the increased appetite, all tell the story of the invigorating benefits of cool, fresh air. Most babies dislike heavy veils, and they may be avoided by a fold of the blanket arranged as a protection shield from the wind.
The wind shield, procurable wherever baby carriages are sold, should be a part of the outdoor equipment, as it greatly helps in the protection of the baby.
The wind should never blow in his face; neither should he lie, unprotected, asleep or awake to gaze up into the sunshine or the sky—or even at a white lining of the hood of his carriage. The lining should be a shade of green, preferably dark green. And while it may be necessary during the summer to suspend a netting over the carriage to protect from flies, mosquitoes, etc., it should never lie on his face.
Many of our readers recall with sadness of heart a little hunchback child or a life-long invalid confined to a bed or wheel chair because some careless but well-meaning caretaker or mother left an open window unguarded; and—in an unlooked for moment—baby crawled too near, leaned out too far, and fell to the ground. The little fellow was picked up crippled for life; and so while it is very essential to baby's health to have open windows, admitting fresh air, they should be amply guarded. Screens afford protection if well fastened, and in their absence a slat three inches wide and one inch thick may be securely fastened across the opening, thus preventing all such tragedies with their life-long regrets.
If any of our readers have seen a new-born baby immediately after he has been washed, dressed, and comfortably217 warmed, they have observed that he usually goes to sleep at once, and that he generally sleeps from four to six hours. Babies, especially new-born babies, need just four things: warmth, food, water, and sleep.
And while the babies sleep they are not to be disturbed by the fond mother's caresses and cuddling—feeling of the tiny hands, smoothing out the soft cheek, or stroking his silky hair—for all such mothers are truly sowing for future trouble. Let baby absolutely alone while sleeping, and let this rule be maintained even if some important guest must be disappointed. If such cannot wait till baby wakens, then he must be content with the mental picture drawn from the mother's vivid description of baby—his first smile, his first tooth, his first recognition of the light, etc. The wise mother cat never disturbs her sleeping kittens.
Sleeping, eating, and growing occupy the whole time of young babies. Until they are two months old they need from eighteen to twenty hours sleep out of each twenty-four; and not less than sixteen hours up to the end of the first year.
At six months, baby should sleep right through the night from six in the evening until six in the morning, with a ten o'clock feed, which should be given quietly, in a darkened room, the babe being immediately returned to his bed.
At two or three years of age, twelve to fourteen hours of sleep is required; while at four to five years, eleven to twelve hours are needed; when they attain the age of thirteen years they should still have ten hours of unbroken sleep each night.
As a general rule, children should sleep alone; even in the case of two brothers or two sisters, separate beds are far better than a double bed for both hygienic and moral reasons.
Baby should have a separate bed. The temptation to nurse him on the least provocation, as well as the danger of overlying, are reasons enough for such an arrangement.
At five-thirty in the afternoon, baby should be undressed, rubbed or bathed, made perfectly comfortable, and fed; then,218 my mother reader, he should be laid down in his little bed and allowed to go to sleep, without any coaxing, singing, rocking, or even holding his hand. Babies will do this very thing and continue to do it if you never begin to rock, jolt, bounce, or sing to them; and, mind you, if you do sing to them or rock them, or even sit near without doing anything but "just hold their tiny hands," there will come a time when you greatly desire to do something else—you have many urgent duties awaiting you—and baby not being old enough to understand the circumstances, begins to wail out his feeling of neglect and abuse. It is nothing short of wicked thus to spoil a child.
We have seen so many beautiful babies go to sleep by themselves without any patting, dangling, or rocking, that we encourage and urge every mother to begin right, for if the little one never knows anything about rocking and pattings he will never miss them; and even if the baby is spoiled through extra attention which sickness often makes necessary, then at the first observance of the tendency on the part of the child to insist on the rocking, or the presence of a light in the sleeping-room, or the craving for a pacifier, we most strongly urge the mothers to stick to the heroic work of "letting him cry it out."
The notion that the household must move about on tiptoes is not only unnecessary but perfectly ridiculous. From the very hour of his birth, let the child become accustomed to the ordinary noises of the home, and if this plan is early started he will prove a blessing and a ray of sunshine to the family and not an autocrat to whom all must bow and bend the knee.
Bedtime is regulated somewhat by the hour of rising in the morning. Usually, up to two years, baby is put to bed from five to six p. m. Regularity is urged in maintaining the bedtime hour.
The seven o'clock bedtime hour is later established and continued until the young child attains school age, when retiring at the curfew hour of eight o'clock gives our boy or girl from ten to eleven hours of sleep, which is essential to proper growth, calm nerves, and an unruffled temper.219
The first few days finds our little fellow sleeping nine-tenths of his time. Let him lie on his right side, for this favors the complete closure of the fetal heart valve, the foramen ovale.
Whether baby lies on his stomach, his side, or with the hands over his head is of little or no consequence. His position should be changed first from one side to the other until he is old enough to turn himself.
Before baby is three months old, he should receive nourishment during the night at nine and twelve, and again at six in the morning. After four or five months a healthy child should not be fed between the hours of ten p. m. and six a. m. At this age, many children sleep right through from six p. m. to six a. m. without food.
After five months, if a healthy baby awakens between ten p. m. and six a. m. warm water may be given from a bottle; he soon forgets about this and the night's sleep becomes unbroken. There are many other reasons than the need of food that cause the wakefulness of the child; and since the baby should, after a few months, sleep undisturbed and peacefully, if he is wakeful and restless—crying out in a peevish whine—and then quiets down for a few moments only to cry out again, you may suspect one of a half-dozen different things. Let us, therefore, summarize the things which may disturb baby's sleep:
1. Lack of Fresh Air. Babies cannot sleep peacefully in a hot, stuffy room, or in a room filled with the fumes of an oil lamp turned low. A crying fretful baby often quiets down as if by magic, providing he is not hungry and the diaper is dry, when taken into a cool room with fresh air. After the first two months the temperature of the sleeping room should be fairly cool and fresh.
2. Clothes and Bedding. The night clothes may be irritating and causing perspiration, while the bedding may be wrapped too snugly about the child. If baby's neck is warm and moist, you may know that he is too warm. If the diaper is wet it should be changed at once. One of the worst habits a baby can possibly get into is to become so accustomed to a wet diaper that220 it does not annoy him. In cold weather he is changed under the bed clothing without exposure or chilling. It may be the bedding is cold and, if so, it should be warmed up by the use of the photophore previously described, or by means of the flannel-covered hot water bottle.
3. The Food. Too little, too much, or the wrong kind of food, will disturb baby's sleep. Indigestion is very easily produced in babies who are improperly fed. For instance, the mother's milk may be lacking in nourishment and baby may really be hungry; or, as in the case of a bottle-fed baby, it is usually due to over feeding. Many mothers we have known who sleep with their babies or who sleep very near them, nurse them every time they wake up or murmur, and this soon becomes one of the biggest causes of disturbed sleep.
4. Spoiling. A lighted nursery or bedroom, rocking to sleep, jolting the carriage over a door sill or up and down, the habit of picking baby up the moment he cries, late rompings—any and all of these may disturb sleep, as well as unsettle the tender nervous system of the child, thus laying the foundation for future nervousness, neurasthenia, and possibly hysteria. This is particularly true in the case of the children who have nervous parents.
5. Reflex Causes. Wakefulness is sometimes due to reflex nervous causes such as the need for circumcision, or the presence of adenoids, enlarged tonsils or worms. Does baby have to breathe through his mouth? Then you may suspect adenoids or other conditions which should be removed.
6. Chronic Disorders. The presence of scurvy or syphilis causes the child to cry out sharply as if in acute pain, while in older children tuberculosis of the spine or hip is attended by a sharp, painful crying out during sleep. Malnutrition or anemia are also conditions which greatly disturb sleep.
7. Soothing Syrups. Untold trouble, both physical and nervous, is bound to follow the giving of soothing syrups. These medicines soothe by knocking the nerves senseless and never by removing the cause. They contain morphin, opium, cocain, heroin, and other drugs which deaden pain, and are most dangerous to give baby.221
The morning nap from the sixth month on should be from two to three hours long, out on the porch, well protected; while the afternoon nap may be from one to one and a half hours long with an interval of two or three hours before bedtime. The child should be wakened at regular intervals for feedings during the day—every three hours until he is six months old, and then every four hours. These naps should be taken in a cool place—on the porch, on the roof, in the yard, under a tree, or on the protected fire escape.
If the nap is to be taken indoors, then lower the windows from the top and darken the room. All children should take daily naps until they are five or six years old.
Possibly if all our babies could grow up in a mild, warm climate, out of doors, where they were cared for by mothers who had nothing else to do but enjoy nature in a garden, their babies unhampered by clothes and other conventionalities inflicted upon us by our present standards of living—well, if that were our environment, probably this chapter on baby hygiene would not need to be written. But realizing that variable climatic conditions, the indoor life, and the necessary bundling up with clothes, all tend to increase the ever-present danger of infection from thickly settled peoples and their domestic pets—these facts, together with the further fact that modern social conditions make it necessary for some mothers to toil long hours—all these influences, I say, considered separately or combined, make it imperative for us to give thoroughgoing consideration to the essentials of baby hygiene. The subjects of fresh air, sleep, bathing, etc., have been duly discussed in previous chapters.
As soon as the newborn baby has been washed and dressed, before he is put to sleep, he is given two teaspoons of warm, boiled water in a sterile bottle with a clean nipple. This is repeated every two hours when he is awake, until he is old enough to ask for water himself. This water should contain no sugar, or anything else—just clean, boiled water. It is better to give this water from a bottle; for in case of enforced weaning, this practice of taking his water from a bottle, will have made him acquainted with that method of feeding.223
The baby may pass very little urine during the first day or two of his life, but if the warm, boiled water is administered regularly, the urine will soon become more abundant.
As the child nears two years of age, if put to bed at six p. m. he should be taken up at ten or eleven to urinate.
In older children, bed wetting is often corrected by serving the last meal not later than four p. m. and not allowing any liquids after that hour.
The physician should be consulted in all instances where the habit of bed wetting extends beyond three years. The subject will be treated more fully in a later chapter.
A baby pen, lifted up from the floor, well protected at the sides, and covered with mosquito bar—if exposed to flies or mosquitoes—affords splendid opportunity for exercise. Here the little fellow may lay on a well-padded mattress and kick, move his arms, and otherwise roll about to his own satisfaction. It should not be in the direct sunshine, but rather in a protected, somewhat shady place, yet where the air is pure and fresh.
Much exercise is obtained from the daily cry. Here, the arms, legs, hands and feet, as well as the body, are all exercised until the baby is pink. A good rebound of blood is flowing through the well-warmed skin, while the baby is greatly benefited by such daily exercise.
Later on, "creeping" is urged, but not forced. With regard to standing—he will pull himself up on his feet just as soon as nature qualifies him, and so he needs no urging or coaxing in this matter. Older children should be encouraged in active romping, games, etc., rather than to spend the entire day in the more sedentary amusements, puzzle pictures, etc.
It is a most abnormal situation when a three-, or four-year-old child is content to sit quietly all day. There is usually something seriously wrong with a child who never soils his rompers, who never makes a noise, and who does not seem to enjoy normal play and fun.224
Let the little folks early learn that the home is theirs to enjoy and that their little friends are welcome; and thus you may be spared such a reproof as one little lad of four unknowingly gave his mamma. His little friend was approaching the stairs of the play room, when the thoughtless mother carelessly and impatiently remarked: "Oh, are you going to bring Ned upstairs? you'll make so much noise." The little host met his friend at the top with the words: "They don't want boys in the house, we'd better go outdoors." The mother "woke up" and arranged a little "party" upstairs for the two husky, healthy—and noisy—boys.
During the creeping days remember that the floor is the coolest part of the room, and in the absence of the creeping pen, which is "built up" two feet above the floor, extra clothing should be put upon the child while on the floor. During the damp days of early spring and the cool days of late fall, as well as on the bleak days of winter, baby is better off if he is kept off the floor. It is a fine plan to put a number of table boards on top of the springs of the baby's bed; in this way a sort of pen is produced which is high above the cold floor and the baby is content to spend much of his time in this little pen, happy with his playthings.
We most strongly protest against the haphazard, promiscuous kissing of babies. Many forms of disease, such as tuberculosis, syphilis, diphtheria, influenza, common colds, etc., may be carried to the child in this way.
The baby, notwithstanding his attractiveness, his beauty, and his grace, should not be overfondled. Kissing the hand is not much better than the mouth, for the hand quickly finds its way to the mouth. If it be necessary to kiss a baby, then let the kissing be done on the back of the neck or on top of his head, but never on the face or hand.
There came into the office one day a woman forty or more years of age, whose mouth was markedly disfigured, and on my225 inquiring as to the probable cause she said: "Doctor, it is the result of sucking my thumb when I was a mere child, too young to know better, and every time I look into the glass, which I assure you is only when I am compelled to, I curse my parents for not breaking me of that habit." The indulgent parents were hated and despised for neglecting their duty, because of the disfigurement which resulted from this unrestrained habit of early childhood.
Thumb sucking, finger sucking, or pacifier sucking, are all filthy habits, and should be early discouraged. To aid in overcoming the habit of sucking the thumb or biting the fingernails, the ends of the fingers and edges of the nails may be painted with a solution of aloes or quinine. In extreme cases, a splint may be placed on the anterior bend of the elbow, thus preventing the possibility of raising the hand to the mouth.
The "sugar teat" of our mother's generation has passed, as has also the "mumbling" of food for the young child; we no longer give the babies concentrated sugar, nor do we "chew" our children's food at the table.
Extreme cases of chalk or dirt eating have been noted; such tendencies are decidedly abnormal, and require medical attention.
Much colic and fretfulness may be avoided if baby is kept warm. The finger tips are a good thermometer, for if they are warm the feet usually are. "Bundling" is unnecessary, but careful attention should be paid to keeping the feet and hands warm without making the child sweat; that is an art, and all mothers should attain it. An extra flannel wrapper and a pair of heavy wool booties in the winter are good warmth producers. Cotton flannel petticoats should be replaced by warm woolen ones, and when the baby begins to get about on his hands and knees a pair of loosely fitting wool tights, made from discarded woolen underwear are of inestimable comfort and value. In the effort to avoid draughts and body chilling, ever bear in mind baby's need of fresh air and the dangers of sweating, for the sudden cooling of a sweating child is a forerunner of pneumonia, cold catching, diarrhoea, and other troubles.226
During early infancy, baby's temperature sometimes varies greatly; for instance, a rectal temperature may register 97.5 or 100.5 F. while the child may be in perfectly good health.
The baby's temperature should be taken at the rectum—which should normally register 99.5 F. This temperature, as stated above, may register 100.5 F., with no other symptoms of illness. In taking rectal temperature the thermometer should remain in place two minutes.
The groin is the next best place to take the temperature; here the thermometer should remain five minutes, and the registry is usually a degree lower than that of the rectum.
The baby's temperature usually is a good guide to the severity of any illness. In case the temperature runs above 101 F. the physician should always be notified and his orders carefully followed. Slight causes often produce a high temperature of 103 to 105 F. for a short time; but such a temperature of long duration means serious trouble and demands expert advice and attention. Abnormal temperature will be more fully considered in that section of this work entitled "Common Disorders of Infancy."
The common custom of bouncing or trotting baby on the knee is a harmful one. The young and growing nervous system of the child is decidedly injured by this constant jolting and jiggling, to say nothing of the "spoiling" effects of this practice. There is a vast difference between the sensitive nervous system of the infant, with its liability to shock and disturbances, and that of the settled and developed nervous system of an adult. The strength of the mother or nurse is so great that the jarring not only often causes indigestion and vomiting in the infant, but sometimes also lays the foundation for "wrecked nerves" in later life.
The tossing of baby in the air comes in for the same condemnation. Baby is not "our plaything," and must not be bounced and tossed about like a rubber ball.227
The first carriage should be roomy and comfortable. The bed should be thirty-three inches long and fourteen inches wide, and should be twenty-eight or thirty inches from the floor. The wheels should be rubber tired. The cover should be a good sized hood containing a dark lining, and provided with a wind shield. This dark lining creates a neutral shade for the eyes and protects them from the glare of the sun and the bright skies.
The bed of the carriage should be soft and warm; and, with the size before mentioned, there is ample room for the "tucking in" with warm blankets, which are first spread out on the bed and then the baby placed into the blanket, after which it is brought up and over him.
The folding go-cart and the small carrying-basket are to be used only in an emergency. They are convenient in traveling or shopping for the mother who has no maid or caretaker with whom to leave the baby; but they are not satisfactory pleasure vehicles, neither should the baby be left to sit fastened in one of these carts for any great length of time.
The mattress of the carriage should be of hair, while needed warmth may be secured by the use of a thick, light-weight woolen blanket, placed under the child and brought up and around him.
A top covering for the carriage must have washing or dry cleaning qualities. A crocheted afghan, a washable embroidered cover, or a firm silk puff, are good covers. The one thing to be remembered is that everything about the carriage soils readily, and if this thought enters into the selection of fabrics, you will not be disappointed when cleaning time comes.
The carriage pillow should be of down, except in the very hot months, when hair is preferable. Simple, easily laundered slips may be made from two men's-size handkerchiefs.
Particularly in boys and men, bow legs are not only awkward but are a noticeable deformity; even the little folks notice them and often remark about it, as did one child who sat profoundly eyeing a very important visitor who stood before the cheerfully228 lighted grate warming himself. The little fellow suddenly exclaimed, "Oh, Mister, look out! You're warping." Such a painful experience might have been saved this distinguished gentleman had his mother or caretaker not urged his standing too soon; and at the same time had fed him on the proper food, so as to avoid "rickets." The ossification or hardening of the bones of the legs continues all through childhood and is often interfered with by improper feeding during the first two years of life. Urging the little people to stand too early is to be discouraged. Nature prepares them for it when the right time comes; which time varies—thin children standing and walking usually much earlier than heavy children.
A very young baby should be lifted from his bed by grasping the clothing below the feet with the right hand, while the left hand slips underneath the back and with spreading fingers supports the neck and head. It is then raised upon the left arm. During the early months the entire spine must be supported in this manner (See Fig. 6). In grasping a baby under the arms or about the waist, undue pressure is made upon the abdomen and chest. Serious injury often follows the careless lifting of the older child by his wrists or hands. The throwing or whirling of the older children by the arms is strongly condemned. Dislocations have followed such careless so-called fun.
In the selection of the high chair, care should be given to the possibility of overturning. Fortunately, baby's bones are only partially ossified, else he would sustain many fractures in the frequent falls and bumps. When we pause to consider the thoughtless manner in which many babies are left on beds and in unguarded chairs, it is not strange that they fall so often.
Open windows must be carefully protected by well-fastened screens or by slats of wood. Beds afford a good place for a romp or play, but high-backed chairs should be placed at the side to prevent a fall. A strap across the waist should be fastened to the sides of the carriage to prevent falling out. Every229thing possible should be done to prevent falls. Outdoor hammocks are exceedingly dangerous for the baby. Never leave a child in one unguarded. A little caution, a large amount of common sense—the "good use of brains"—will prevent scars and other lifelong deformities.
Never allow anyone to manipulate or "break down" a swollen breast in a girl or boy baby during the first week or two. This swelling occurs often and should not be interfered with. A hot compress of boracic acid solution may be applied, after which a piece of sterile gauze should be placed over the swollen part and held on by a muslin bandage. Secure medical attention if the swelling does not go down in a day or two.
Unless absolutely necessary, babies should not be taken on trains and street cars; nor should they take long journeys into the country to attend "reunions." Infections accompany crowds, and baby is far better off at home, in the quiet of his natural surroundings, than he is in the dust, closeness, and bustle of illy ventilated cars, streets, shops, movies, or even at church. Many an infant has been sacrificed by a train journey to "show him off" to the fond grandparents; scores of babies acquire whooping cough at the movies; and many a baby has nearly lost his life by catching measles, scarlet fever, or diphtheria at church; while the only thing accomplished by the church experiment was the spoiling of the entire service by its fretful, tired cry—the infant's only means of protest.
"Runabouts" are the little folks between the age of one and three years, and they require good care, good feeding, and warm and comfortable dressing.
In general, they need the same fresh air, daily outings, and daily naps of the younger child. Their hands need washing oftener, and their clothing, which is usually a play romper, should be either of white or fast colors that it may be most thor230oughly boiled, thus getting a good disinfection. Their eyes, nose, and ears, as well as the genital organs, all require the most rigid daily cleanliness.
The "bugbear" second summer need not be feared by the mother who takes particular care to see that:
The second summer is no harder than the first, as good clean water, easily digested foods, and good general hygiene are all a baby needs at this time. A large army of little folks grow up in spite of the little care they get and the place in which they live. Did they not possess good vital resistance, sound nerves, and good digestion, the children of the "slums" and of the "ghetto" would quickly succumb to their unhygienic surroundings.
In selecting toys for the infant, it must be borne in mind that they will be put to the mouth, and hence they should not be:
Bear in mind that babies are easily amused with such simple toys as:231
The older children have wonderfully good times out of doors with a spade, a cart, and the sandpile. Boys most thoroughly enjoy a track with its engine and cars, switches, etc. They build sham fortifications, truly works of art, with their blocks, while the girls are happiest with dolls and household sets. However, occasionally we meet a mother who has a girl who is really a boy in her tastes for toys, and so we say to that mother: give the little girl the desire of her heart; if it's a train instead of a doll, or a toy gun instead of a doll's trunk, well and good, let her have them. What we want are free and easy, natural, children. They are much more likely to have good nerves, clean thoughts, sound digestion, and equalized circulation.
The newborn baby comes into the world in an absolutely helpless condition and completely unconscious of his surroundings. He unconsciously performs certain acts, such as opening his eyes, crying, urination, movement of the bowels, and even nursing of the breast; but there is probably no distinct voluntary action connected with any of these acts. All of his senses at birth are practically dormant, but as the days and weeks go by, they begin to awaken.
The baby cries, but the tears do not actually flow over the lids until he is three or four months old, and while the baby may fix his eyes upon objects and distinguish light from darkness, he will not wink nor blink when the finger is brought close to the eye. Vision is probably not complete until the beginning of the third month.
Infants are said to be deaf for the first twenty-four to forty-eight hours after birth, and some authorities hold that they are deaf for several days.
Taste is early developed, as a newborn baby will often repeatedly show a desire to taste sweet things, while if sour or bitter things are put to the tongue, it shows its displeasure.
The newborn baby usually comes into the world with a good head of hair, but the end of the first or second week witnesses the falling out of much of this hair, and falling may continue for even another week or two. The hair is often worn off on the back of the head because of constant friction upon the pillow.233
Children differ greatly in the growth of hair. Some of them come into the world with heavy hair, and others lose it quickly and remain nearly bald-headed until after the first year.
As the second hair grows in, it is usually lighter than it was at birth and lighter than it will be later in life, as the hair has a tendency to grow darker as the years go by.
The scalp should receive the care already mentioned. As the hair comes in it should be shampooed once in two weeks and brushed often, making it healthy and vigorous.
It is wise to turn the baby first on one side and then on the other and not allow him to sleep night after night on one side of his head. The newborn head may be misshapen by laying the child constantly on one side, and the ear may be misshapen if it is allowed to curl under or become pressed forward. Markedly protruding ears may be partially corrected by having the child wear a well-ventilated cap made for the purpose.
Many mothers think that the presence of drooling or the excessive flow of saliva is associated with teeth cutting. While it may be associated with the teeth, this is not usually the case; it is more probably due to the beginning of a new function of secretion. The newborn baby has only enough saliva to furnish moisture for the mouth, and not until the age of four or five months does saliva really flow, and since the teeth appear a bit later we often confuse the institution of a new secretion with the oncoming teeth.
The young baby manifests a number of sensations early in its career. Hunger and satisfaction as well as comfort and discomfort seem to be recognized by the little fellow. He early learns that the approach of someone when he cries usually means that he is to be taken up, and he usually ceases crying as soon as he is taken up. He early manifests a sense of comfort when he is cuddled; there also is early234 present a manifestation of the desire to sleep, and the satisfying pleasure of a drink of water.
At the age of three months he has recognized many things such as the light or a bright object. He distinctly recognizes his mother and often smiles at her approach. He recognizes his hands at four months, and now begins to recognize other members of the household aside from his mother. Even as early as one month, he may smile at his mother. At two months of age he will often smile at other members of the family. He laughs out loud or chuckles during the fourth or fifth month. But, on the whole, he must be considered as just a little animal whose greatest needs are to have his appetite and thirst satisfied, his little body clothed, and his little nerves put to rest—to sleep.
At four months the normal baby will hold up his head; and if he is supported at the back with a pillow, he will sit erectly—holding his head up—at six months; while at eight months or not later than nine, the normal child should sit alone on the floor with no support. Later in the ninth month he often manifests a desire to bear his weight upon his feet. Care is here urged that the mother protect the little fellow at this time and not allow him to rest his weight upon his feet but a moment or two at a time.
He will reach for a ball suspended from the top of his carriage or bed as early as the fifth month. About this time he discovers his toes while in his bath. He will handle a rattle at six or seven months, and shows delight in such toys.
In both the upper and lower jawbones of the newborn infant there are hidden away in snug little cavities two sets of tiny teeth; the first set, or milk teeth, and the second set, or permanent teeth. These rudimentary teeth grow as the baby grows and push their way up or down from the jawbones until they finally make their appearance through the gums. The milk teeth appear in a definite way and in five definite groups.235
There should be no physical disturbance at the appearance of the teeth, which is a physiological process, and it is to be deplored that all of the ills of babyhood are laid upon the teeth with the careless remark: "Oh, its his teeth!" Many, many illnesses are neglected because our inexperienced mother has been told that she can expect "anything to happen when the baby is cutting its teeth." Now, it is true that the babies of many families do have trouble in cutting their teeth, but the majority of babies cut their teeth comfortably and the first knowledge anyone has of it is the appearance of the tooth itself. As the teeth push their way nearer the surface of the gums, there is a broadening and a hardening of the gums themselves, and it is the exception rather than the rule that the baby needs any help in cutting his teeth.
Usually by the time the baby is seven months old it has two central teeth on the lower jaw (the central incisors), which constitute the first group. The second group of teeth to appear is the four upper central teeth which are all through by the time the baby is twelve months old, and are often through at ten months. Then there is a pause of from one to three months before the next teeth appear—the four anterior molars. As these four anterior molars come in, the two lateral incisors appear on the lower jaw, which now gives us, by the time the baby is fourteen or fifteen months old, four central teeth upper, four central teeth lower, and the four anterior molars, which make twelve teeth.
Another pause of two or three months and then we get the four canine, which fill in the space between the first molars and the front teeth. The canine on the upper jaw are commonly known as the eye teeth, while the canine teeth on the lower jaw are spoken of as the stomach teeth. This brings us to the age of eighteen to twenty-four months, when there is still another pause of two or three months, after which time the big teeth or the four posterior molars appear, which completes the first set of twenty teeth—the milk teeth. When baby is twenty months old the milk teeth are often all in. The complete set should appear not later than the thirtieth month.
During the life of the milk teeth the child should be taken236 to the dentist at least once a year, better once in six months, for all defective teeth must be properly and promptly cared for. Inexpensive but sanitary fillings should be placed in all decayed teeth, for the roots of the first teeth are very soft and infection readily spreads to the jaws and the permanent teeth and serious trouble often begins thus early.
If dentition is seriously delayed, investigation should be started concerning the general condition of the child, for this delay often accompanies ill health.
When the child is six years old, the mother should be watchful, for it is at this time that the first permanent teeth appear just behind the last molar of the milk teeth. They do not replace any of the teeth present, and many times they come through and decay without receiving any attention. It is seldom necessary to assist these milk teeth as they come through the gum, and should the gums become highly colored and swollen it is not wise to lance them, for if the teeth are not ready to come through immediately, the gum only toughens the more and makes the real cutting still more painful.
This is the time to cut down the baby's food as well as to look for other digestive disturbances, for the number of stools may increase and vomiting may occur, and by reducing the quantity and quality of the food and encouraging abundant water drinking, much trouble may be avoided. Under no circumstances urge the baby to eat when he refuses his food, when the gums seem swollen and red during the teething time. You will find that he will enjoy orange juice, pineapple juice, or prune juice. All of these digestive symptoms are simply the result of "feeling bad," and if heavy food of his regular feeding is greatly diminished he will get along much better than if fed his regular allowance of food.
The normal child has:
Six teeth at one year.
Twelve teeth at one and one-half years.
Sixteen teeth at two years.
Twenty teeth at two and one-half years.
237
When the child is six years old the first permanent tooth appears just back of the last of the milk teeth. By the time he is seven, the four central teeth, two above and two below, are out and the new ones begin to appear. The order of their appearances is as follows:
| Four first molars | 6 years |
| Four central incisors | 7 years |
| Four lateral incisors | 8 years |
| Four first bicuspids | 9 to 10 years |
| Four second bicuspids | 10 to 11 years |
| Four canines | 11 to 13 years |
| Four second molars | 12 to 15 years |
| Four third molars | 17 to 25 years |
A better plan than to lance swollen gums is to rub them gently with ice wrapped in a soft cloth, or to dip the finger in ice water and rub the gums—this often gives the baby much relief.
Often the baby finds comfort in biting on an ivory ring, but the utmost care must be used in keeping it clean and avoiding contamination by allowing it to drop on the floor.
Convulsions are never the symptoms of teething. Consult a physician at once, as such seizures probably spring from causes other than teething.
Cleansing of the teeth should be carried out systematically every morning by means of a piece of cotton which has been dipped in a boric-acid solution or a solution of bicarbonate of soda (common baking soda). A soft brush may be used for cleansing, and when there are particles of food between the teeth they should be removed by strands of waxed floss.
Throughout life, frequent visits should be made to the dentist; during early childhood days he should be on the lookout for symptoms which indicate deformity—narrow jaws and other conditions which affect the permanent teeth. During adolescence and adult life the teeth should be examined every six months and cleansings of the mouth should become a part of the daily toilet.238
During the first year, nothing gives us so much information concerning the child's general well-being as the weight. Such a record will not only enlighten the mother concerning the development of the child, but the grown-up child appreciates the record and preserves it along with the other archives of babyhood days. Every Sunday morning, when the father is at home, the baby should be weighed and an accurate record kept. It is important that the baby be weighed each time in the same garments—shirt, band, diaper, and stockings—for every ounce must be accounted for.
Until the baby is five or six months old he should gain from four to eight ounces a week. Anything short of this is not enough and should be reported to the physician. After six months the gain is about a pound each month. This varies somewhat; possibly during the tenth and eleventh month the gain is lessened, but by the close of the first year the baby should have trebled its birth weight.
Dr. Griffith gives us the following very interesting bit of information concerning the weight of boys and girls after the first year, and to him also belongs the credit for the accompanying table showing the growth, height, and weight of the child up to sixteen years of age.
After the first year we notice that, taking it all together, there is a gradual increase in the number of pounds and a decrease in the number of inches added yearly, four inches being gained in both the second and third years, three inches in the fourth and fifth years, and after this two inches a year. The gain in weight is four pounds yearly from the age of three to that of seven years, then five, then six, and then about nine pounds. It sometimes happens that at about the age of nine in girls and eleven in boys there is almost a cessation of growth for a short time. Later, at about twelve years, girls take on a particularly rapid growth, and decidedly exceed boys of the same age in weight, and sometimes in height also. At fifteen or sixteen years the rapidity of growth in girls, both in weight and height, will be greatly diminished, while boys of this age will often begin to develop very rapidly, and will soon materially exceed the other sex in both respects.
| Age. | Height. | Weight. | |||
| Birth | 19 inches. | 7 lbs. | 8 oz. | ||
| 1 week | 7 " | 7½ " | |||
| 2 weeks | 7 " | 10½ " | } | Gained 1 oz. a day; 7 oz. a week |
|
| 3 weeks | 8 " | 2 " | |||
| 1 month | 20½ " | 8¾ " | |||
| 2 months | 21 " | 10¾ " | |||
| 3 months | 22 " | 12¼ " | } | { | Gained ¾ oz. a day; 5½ oz. a week |
| 4 months | 23 " | 13¾ " | |||
| 5 months | 23½ " | 15 " | } | { | Double original weight. Gained 2/3 oz. a day; 42/3 oz. a week Gained ½ in. a month Gained about 1 lb. a month Treble original weight. |
| 6 months | 24 " | 16¼ " | |||
| 7 months | 24½ " | 17¼ " | } | ||
| 8 months | 25 " | 18¼ " | |||
| 9 months | 25½ " | 18¾ " | |||
| 10 months | 26 " | 19¾ " | |||
| 11 months | 26½ " | 20½ " | |||
| 1 year | 27 " | 21½ " | |||
| 2 years | 31 " | 27 " | } | { | Gained 4 in. a year |
| 3 years | 35 " | 32 " | |||
| 4 years | 37½ " | 36 " | } | { | Double original length. Gained 3 in. and 4 lbs. a year. |
| 5 years | 40 " | 40 " | |||
| 6 years | 43 " | 44 " | } | { | Gained 2 in. and 4 lbs. a year. |
| 7 years | 45 " | 48 " | |||
| 8 years | 47 " | 53 " | } | { | Gained 2 in. and 5 lbs. a year. |
| 9 years | 49 " | 58 " | |||
| 10 years | 51 " | 64 " | } | { | Gained 2 in. and 6 lbs. a year. |
| 11 years | 53 " | 70 " | |||
| 12 years | 55 " | 79 " | } | ||
| 13 years | 57 " | 88 " | |||
| 14 years | 59 " | 100 " | { | Gained 2 inches and about 9 lbs. a year. |
|
| 15 years | 61 " | 109 " | |||
| 16 years | 63 " | 117 " |
The accompanying illustration (Fig. 14), taken from Dr. Yale, represents the developmental changes at one, five, nine, thirteen, seventeen, and twenty-one years. Each figure is divided into four equal parts, and as we watch the development from the baby who at one year, as Dr. Yale says, is four heads high, at the age of twenty-one the legs and the trunk have much outgrown the growth of the head, so that at this age the head is only two-thirteenths or less of the whole length of the body. The legs have grown more rapidly and equal one-half the entire body length. The trunk has not kept pace with the legs, for as you will see from the diagram the line reaches the navel of the child in one year, while in the adult it is much lower. The rapid growth of the legs is accomplished after nine years of age.
The proportions of the head, chest, and abdomen are exceedingly important in the growing child. At the end of the first year the head, chest, and abdomen are about uniform in circumference. The head may measure one-fourth of an inch more, but the chest and abdomen should both measure eighteen241 inches in circumference at this time. Should the head or the abdomen be two inches larger than the chest; the attention of the physician should be called to it, for either are indicative of conditions that should be carefully investigated.
As a general rule the normal, healthy, breast-fed baby is given a feeding of a bottle each day after he is ten months old. These bottles are increased in number until, by the time the baby is a year old, he is gradually weaned from the breast. Should the ninth month of baby's life arrive in the hot summer months we urge the mothers to continue breast feeding, with possibly the addition of some fruit juices, as noted elsewhere, until early autumn. Under no circumstances should the baby be weaned and compelled to use cow's milk during the season of the year when the risks of contamination are greatest. If the baby is nursed up to the close of his first year he hardly need be trained to use the bottle, but may take his food from a cup. From one to two months should always be consumed in weaning the baby, unless sudden weaning is necessitated by ill health, as noted elsewhere. The baby should have, if possible, from thirty to forty days to accustom himself to cow's milk exclusively.
If the child is weaned slowly there should be no trouble with the breasts, but in the instance of sudden weaning the mother should restrict her liquids, put on a tight breast binder, and for a day or two should take a dose of a saline cathartic, which will assist in taking care of the liquids and thus decrease the secretion of milk.
If the bottle food is agreeing with the baby he should be allowed to use it up to the end of the first year when he will be given whole milk with possibly the addition of a little lime water. We see no reason why the child should give up his bottle during the second year unless other food is refused—unless he will not accept other food than from his bottle—and if you are convinced that he has formed the "bottle habit,"242 then the milk should be put into a tiny cup or glass, and he should learn to sip it along with his solid foods; but if he takes his other foods without any hesitancy, then we know no reason why he should not take his milk in this comfortable manner from his bottle at least two or three feedings each day.
If you desire to wean him from his bottle, serve the first part of it with a spoon from a cup or glass and then give him the remainder in the bottle. The beautiful picture of a big, robust baby lying on his back, knees flexed, both hands holding his beloved bottle still lingers in my mind as one of the pleasant memories of my lad's babyhood days, and at the close of the second year, when the beloved bottle was left behind, I believe I missed something as well as did the lad.
I recall no difficulty with his taking the food from a cup. The success of all normal weanings is due entirely to the fact that it is done gradually and slowly, and under no circumstances should it be roughly and abruptly attempted—particularly in case of the bottle feeding.
Reference is made to this subject in another part of this book—where we went into the detail of keeping the daily record of these physiological occurrences—and it was found that the bowels moved and the bladder was emptied at about the same time each day. Any mother, caretaker, or nurse, who will take the time to keep a daily record of the hours of defecation and urination, will observe the time carefully and will catch the child on nearly every occasion before an accident occurs. Often as early as four months the bowels will move in an infant's chamber at regular times each day. The nurse or mother places this receptacle in her lap and holds the child gently and carefully upon it. A little later it can be made to sit on a special chair prepared for the purpose, and at eight or nine months by careful training the urination can be controlled, and by the end of the first year the diapers ought to be discontinued.
If the child has not learned to control the bladder by the age of two years, medical attention should be called to the fact and remedial measures instituted.243
The baby should begin to talk at one year. He early learns to say "mamma" and "papa," and gradually adds nouns to his vocabulary, so that at eighteen months the normal child should have a vocabulary of one hundred to one hundred and fifty words. As he nears the two-year mark, he has acquired a few simple verbs and he can possibly put three words together, such as, "Willie wants drink." Pronouns come in late, as we all recall that the young child usually speaks of himself by his own name.
Children are born mimics. If you talk baby talk to them, they will talk baby talk back. For instance, a well known author told us just the other day that for many years no other name was given to the sewing machine in his house but the word "mafinge," and not until he went to school did he correct the word "bewhind," for in the nursery he learned the line "wagging their tails bewhind them." Baby talk is very cunning, and often the adult members of the family pick it up and keep it up for years, and only when they are exposed in public, as one mother was on a suburban platform by her four-year-old lad shouting, "Mamma, too-too tain tumin, too-too tain tumin," do they sense their responsibility and realize how difficult it is to form new habits. This poor mother tried in vain to have her little fellow say, as did another little lad two and one-half years old, "Mother, the train's coming; let's get on."
Many words of our beloved language at best are hard to understand; so let us speak correct English to the little folks and they will reward us by speaking good English in return.
If at two years the child makes no attempt at speech, suspicions should be aroused concerning mutism or other serious nervous defects. Medical advice should be sought.
All guttural tones which may be occasioned by adenoids or enlarged tonsils, all lisping, stuttering, or defective speech of all words should be taken in hand at the very start, as they244 are usually overcome by constant repetition of the correct manner of speaking the particular word in question. Children of defective speech need special training, and should in no way be allowed rapidly to repeat little nursery rhymes, as oftentimes this rapid repetition of rhymes by a child with hereditary nervous defects may occasion stuttering or stammering later on.
Special exercise should not be forced upon young children. Physical culture, along with many other things intended for sedentary adults, should never be forced upon little folks who get all of the exercise they need in the many journeys they take building their blocks, sailing their boats, tearing down imaginary houses, making imaginary journeys—from morning until night the little feet are kept busy—never stopping until the sandman comes at sleepy time. Do not yourself attempt to stimulate a child who seems backward. Consult your physician. You had much better put a child out to grow up in the yard by himself with his sandpile than to force calisthenics or advance physical training upon him.
Do not attempt to hasten nature in aiding the child to walk. Let him creep, roll, slide, or even hunch along the floor—wait until he pulls himself to his feet and gradually acquires the art of standing alone. If he is overpersuaded to take "those cute little steps" it may result in bow legs, and then—pity on him when he grows up. Sometimes flat foot is the result of early urging the child to rest the weight of the body upon the undeveloped arch. A defect in the gait or a pigeon toe is hard to bear later on in life. A certain amount of pigeon-toeing is natural and normal. If the baby is heavy he will not attempt to walk at twelve months. He will very likely wait until fourteen or fifteen months. The lighter-weight children sometimes walk as early as eleven months, but they should all be walking at eighteen months, and if not, it is usually indicative of backward mentality.
If the training of the bowels and bladder will replace the245 diapers with drawers, the baby will attempt to walk sooner than when encumbered with a bunglesome bunch of diaper between the thighs. The little fellow runs alone at sixteen months and thoroughly enjoys it, and the wise mother will pay no attention to the small bumps which are going to come plentifully at this particular time.
He discovers his hands at three or four months. At six months he sits alone, plays with simple objects, grasps for objects, and laughs aloud from the third to the fifth month. He says "goo goo" at four or five months. At one year he should stand with support, listen to a watch tick, follow moving objects, know his mother, play little games, such as rolling a ball, should have trebled his birth weight, and have at least six teeth, and should use three words in short sentences. At eighteen months he should say "mamma" spontaneously, walk and run without support, should have quite a vocabulary, should be able to perform small errands like "pick up the book," and should have twelve to sixteen teeth. At two years he should be interested in pictures, able to talk intelligently, and know where his eyes, nose, mouth, hands, and feet are. At three years, he should enumerate the objects in a picture, tell his surname, and repeat a sentence with six words.
In the case of a premature baby or a very delicate child, or as a result of a prolonged illness or a very severe sickness, such as spinal meningitis, the time of these mental and physical developments may all be postponed, while rickets, which will be spoken of later, is often the cause of late sitting, late standing, and late walking.
Milk is the principal article of diet during the second year. It should be given with regularity at distinct intervals of four meals a day. It may be given from the nursing bottle, unless the child has acquired the bottle habit and refuses to eat anything else but the food from his bottle, in which case it should be given from a cup. Beginning with the sixth month, aside246 from his milk, be it breast milk or bottle milk, he is to be given orange juice once each day as well as the broth from spinach and other vegetables. This is necessary to give the child certain salts which are exceedingly essential to the bottle baby.
At the close of the year when he is taking whole milk he should be given arrowroot cracker, strained apple sauce, prune pulp, fig pulp, mashed ripe banana (mashed with a knife), a baked potato with sauce or gravy (avoiding condiments), and a coddled egg. Fruit juices may be added to the diet, such as grape, pineapple, peach, and pear juice. Later in the second year he may be given stale bread and butter, and for desserts he may have cup custard, slightly sweetened junket, and such fruit desserts as baked apple and baked pear.
We do not think it is necessary to give children much meat or meat juices. We appreciate that there is a diversity of opinion upon this subject, but we do not hesitate to say that in the families where meat is little used, the children seem to grow up in the normal manner with sound healthy bodies, sometimes having never tasted it. When meat is used, it should be well cooked to avoid contamination with such parasites as tapeworm and trichina; it should also be well chewed before swallowing, as many of the intestinal disturbances of the older children are due to the swallowing of unmasticated food such as half-chewed banana, chunks of meat, rinds of fruit, and the skins of baked potatoes.
Let the children's diet be simply planned, well cooked, thoroughly masticated, and above all things have regular meal hours, and no "piecing" between meals; and if the mother begins thus early with her little fellow, she will be rewarded some later day by hearing him say to some well-meaning neighbor, who has just given him a delicious cookie or a bit of candy: "Thank you, I will keep it until meal time." Children learn one of the greatest lessons of self control in following the teaching that nothing should pass the lips between meals but water or a fruit-ade. Children in the second year require four meals a day, one of which is usually only the bottle or a cup of milk. These meals are usually taken at six,247 ten, two, and six in the evening. Oftentimes this early six o'clock meal is just a bottle or cup of milk, as may also be the evening meal.
Now, a word about candy. Pure candy is wholesome and nourishing. It is high in calorific value, and children should be allowed to have it if it does not enter the stomach in solutions stronger than ten or fifteen per cent. We can see at a glance that chocolate creams, bonbons, and other soft candies should never be given to children. Candies that they can suck, such as fruit tablets, stick candy, sunshine candy, and other hard confections that are pure, and free from mineral colorings and other concoctions such as are commonly used in the cheaper candies, may safely be given at the close of the meals—but never between meals.
All such articles as tea, coffee, beer, soft candies, condiments, pastries, and fried foods, should be positively avoided in the case of all children under five and six years of age.
The diet from now on will be considered in the chapter "Diet and Nutrition."
To the mother who has passed through the experience of bringing the child into the world is usually given that intuitiveness which helps her in caring for that child when it is well and in recognizing certain symptoms when it is sick. The newborn baby brings with him a large responsibility, but as the weeks pass by his care becomes less and less of a nervous strain, as the routine duties, so nearly alike each day of his little life, have made the task comparatively easy; but when the baby gets sick, particularly if he is under one year of age, and it is impossible for him clearly to make known his wants, and being unable to tell where it hurts or how badly it hurts, the average mother is likely to become somewhat panicky; and this confusion of mind often renders her quite unfit successfully to nurse the sick baby.
It is often wise to secure the services of a trained nurse, and if the family purse will allow such services, a good, sincere, capable, practical nurse should be engaged, for her firm kindness will often accomplish much more than the unintentional irritability and anxious solicitude of an overworked and nervous mother.
Usually the mother not only attempts the care of the sick baby with the long night vigil—often not having the opportunity to take a bath or change her raiment day in and day out—but she often attempts to manage the entire household252 as well, including the getting of the meals and keeping the house cleaned, and it is not to be wondered at that her nerves become overtaxed and in an unlooked for moment she becomes irritable and cross with the sick child.
No matter how low the financial conditions of the family may be, outside help is always essential in cases of severe or long-continued illness of the children. Should the mother insist upon caring for the baby herself, then all household duties should be given over to outside help, and as she takes the rôle of the nurse, the same daily outing and sleep that an outside nurse would receive should be hers to enjoy.
Dr. Griffith has so ably detailed the "features of disease" that we can do no better than to quote the following:[3]
The position assumed in sickness is a matter of importance. A child feverish or in pain is usually very restless even when asleep. When awake it desires constantly to be taken up, put down again, or carried about. Sometimes, however, at the beginning of an acute disease it lies heavy and stupid for a long time. In prolonged illnesses and in severe acute disorders the great exhaustion is shown by the child lying upon its back, with its face turned toward the ceiling, in a condition of complete apathy. It may remain like a log, scarcely breathing for days before death takes place. Perfect immobility may also be seen in children who are entirely unconscious although not exhausted.
A constant tossing off of the covers at night occurs early in rickets, but, of course, is seen in many healthy infants, especially if they are too warmly covered. A baby shows a desire to be propped up with pillows or to sit erect or to be carried in the mother's arms with its head over her shoulder whenever breathing is much interfered with, as in diphtheria of the larynx and in affections of the heart and lungs. The constant assumption of one position or the keeping of one part of the body still, may indicate paralysis. When, however, a cry attends a forcible change of position, it shows that the child was still because movement caused pain.
Sleeping with the mouth open and the head thrown back often attends chronic enlargement of the tonsils and the presence of 253adenoid growths in young children, although it may be seen in other affections which make breathing difficult. In inflammation of the brain the head is often drawn far back and held stiffly so. Sometimes, too, in this disease the child lies upon one side with the back arched, the knees drawn up, and the arms crossed over the chest. A constant burying of the face in the pillow or in the mother's lap occurs in severe inflammation of the eyes.
The gestures are often indicative of disease. Babies frequently place the hands near the seat of pain; thus in slight inflammation of the mouth they tend to put the hand in the mouth; in earache to move it to the ear; and in headache to raise it to the head. In headache or in affections of the brain they sometimes pluck at the hair or the ears, although they may often do this when there is no such trouble. Picking at the nose or at the opening of the bowel is seen in irritation of the intestine from worms or oftener from other cause. A child with a painful disease of its chest may sometimes place its hand on its abdomen, or a hungry child try to put its fists into its mouth.
In approaching convulsions the thumbs are often drawn tightly into the palms of the hands and the toes are stiffly bent or straightened. Very young babies, however, tend to do this, although healthy. The alternate doubling up and straightening of the body, with squirming movements, making of fists, kicking, and crying, are indications of colic. This is especially true if the symptoms come on suddenly and disappear as suddenly, perhaps attended by the expulsion of gas from the bowel.
The color of the skin is often altered in disease. It is yellow in jaundice, and is bluish, especially over the face, in congenital heart disease. There is a purplish tint around the eyes and mouth, with a prominence of the veins of the face, in weakly children or in those with disordered digestion. A pale circle around the mouth accompanies nausea. The skin frequently acquires an earthy hue in chronic diarrhea, and is pale in any condition in which the blood is impoverished, as in Bright's disease, rickets, consumption, or any exhausted state. Flushing of the face accompanies fever, but besides this there is often seen a flushing without fever in older children the subjects of chronic disorders of digestion. Sudden flushing or paling is sometimes seen in disease of the brain.254
The expression of the face varies with the disease. In whooping cough and measles the face is swollen and somewhat flushed, giving the child a heavy, stupid expression. There is also swelling of the face, especially about the eyes, in Bright's disease. Repeated momentary crossing of the eyes often indicates approaching convulsions. In very severe acute diarrhea it is astonishing with what rapidity the face will become sunken and shriveled, and so covered with deep lines that the baby is almost unrecognizable. The same thing occurs more slowly in the condition commonly known as marasmus. Often the face has an expression of distress in the beginning of any serious disease. If the edges of the nostrils move in and out with breathing, we may suspect some difficulty of respiration, such as attends pneumonia. The baby sleeps with its eyes half open in exhausted conditions or when suffering pain.
The head exhibits certain noteworthy features. Excessive perspiration when sleeping is an early symptom of rickets. It must be remembered, however, that any debilitated child may perspire more or less when asleep. Both in rickets and in hydrocephalus (water on the brain) the face seems small and the head large, but in the former the head is square and flat on top, while in the latter it is of a somewhat globular shape. The fontanelle is prominent and throbs forcibly in inflammation of the brain, is too large in rickets and hydrocephalus, bulges in the latter affection, and sometimes sinks in conditions with only slight debility.
The chest exhibits a heaving movement with a drawing in of the spaces between the ribs in any disease in which breathing is difficult. A chicken-breasted chest is seen in Pott's disease of the spine, and to some extent in bad cases of enlargement of the tonsillar tissue; a "violin-shaped" chest in rickets; a bulging of one side in pleurisy with fluid; and a long, narrow chest, with a general flattening of the upper part, in older children predisposed to consumption.
The abdomen is swollen and hard in colic. It is also much distended with gas in rickets, and is constantly so in chronic indiges255tion in later childhood. It is usually much sunken in inflammation of the brain or in severe exhausting diarrhea or marasmus. It may be distended with liquid in some cases of dropsy.
The study of the cry furnishes one of the most valuable means of learning what ails a baby. A persistent cry may be produced by the intense, constant itching of eczema.
The paroxysmal cry, very severe for a time and then ceasing absolutely, is probably due to colic, particularly if accompanied by the distention of the abdomen and the movements of the body already referred to. A frequent, peevish, whining cry is heard in children with general poor health or discomfort. A single shrill scream uttered now and then is often heard in inflammation of the brain. In any disease in which there is difficulty in getting enough air into the lungs, as in pneumonia, the cry is usually very short and the child cries but little, because it cannot hold its breath long enough for it. A nasal cry occurs with cold in the head.
A short cry immediately after coughing indicates that the cough hurts the chest. Crying when the bowels are moved shows that there is pain at that time. A child of from two to six years, waking at night with violent screaming, is probably suffering from night terrors. In conditions of very great weakness and exhaustion the baby moans feebly, or it may twist its face into the position for crying, but emit no sound at all. This latter is also true in some cases of inflammation of the larynx, while in other cases the cry is hoarse or croupy. Crying when anything goes into the mouth makes one suspect some trouble there. If it occurs with swallowing, it is probable that the throat is inflamed.
With the act of crying there ought always to be tears in children over three or four months of age. If there are none, serious disease is indicated, and their reappearance is then a good sign.
The character of the cough is also instructive. A frequent, loud, nearly painless cough, at first tight and later loose, is heard in bronchitis. A short, tight, suppressed cough, which is followed by a grimace, and, perhaps, by a cry, indicates some inflammation about the chest, often pneumonia. There is a brazen, barking, "croupy" cough in spasmodic croup. In inflammation of the larynx, including true croup, the cough may be hoarse, croupy, or sometimes almost noiseless.256
The cough of whooping cough is so peculiar that it must be described separately when considering this disease. Then there are certain coughs which are purely nervous or dependent upon remote affections. Thus the so-called "stomach cough" is caused by some irritation of the stomach or bowels. It is not nearly so frequent as mothers suppose. Irritation about the nose or the canal of the ears sometimes induces a cough in a similar way. Enlarged tonsils or elongated palate or throat irritation may also produce a cough.
The breathing of a young child, particularly if under one year of age and awake, is always slightly irregular. If it becomes very decidedly so, we suspect disease, particularly of the brain. A combination of long pauses, lasting half a minute or a minute, with breathing which is at first very faint, gradually becomes more and more deep, and then slowly dies away entirely, goes by the name of "Cheyne-Stokes respiration," and is found in affections of the brain. It is one of the worst of symptoms except in infancy, and even then it is very serious.
The rate of respiration is increased in fever in proportion to the height of the temperature. It is increased also by pain in rickets, and especially in some affections of the lungs. Sixty respirations a minute are not at all excessive for a child of two years with pneumonia, and the speed is frequently decidedly greater than this.
Breathing is often very slow in disease of the brain, particularly tubercular meningitis. Poisoning by opiates produces the same effect. Frequent deep sighing or yawning occurs in affections of the brain, in faintness, or in great exhaustion, and may be a very unfavorable symptom. Breathing entirely through the mouth shows that the nose is completely blocked, while snuffling breathing is the result of a partial catarrhal obstruction. A gurgling in the throat not accompanied by cough may indicate that there is mucus in the back part of it, the result of an inflammation, sometimes slight, sometimes serious.
"Labored" breathing, in which the chest is pulled up with each breath while the muscles of the neck become tense, the pit of the stomach and the spaces between the ribs sink in, and the edges of the nostrils move in and out, is seen in conditions where the natural ease of respiration is greatly interfered with, as in pneumonia, diphtheria of the larynx, asthma, and the like. Long-drawn, noisy inspirations and expirations are heard in obstruction of the larynx, as from laryngeal diphtheria or spasmodic croup.257
The rate of the pulse is subject to such variations in infants that its examination is of less value than it would otherwise be. In early childhood its observation is of more service, although even then deceptive. Slight irregularity is not uncommon. Unusual irregularity is an important symptom in affections of the brain or heart. Fever produces an increase in the pulse rate, the degree of which depends, as a rule, upon the height of the temperature. Slowing of the pulse is a very significant symptom, seen particularly in affections of the brain, and sometimes in Bright's disease and jaundice.
The temperature is of all things important to remember in infancy and childhood because fever is easily produced and runs high from slight causes.
Even slight cold or the presence of constipation or slight disturbances of digestion may in babies sometimes produce a temperature of 103 F. or more. We do not speak of fever unless the elevation reaches 100 F. A temperature of 102 or 103 F. constitutes moderate fever, while that of 104 or 105 F. is high fever, and above 105 F. very high. A temperature of 107 F. is very dangerous, and is usually not recovered from. The danger from fever depends not only upon its height, but upon its duration also. An elevation of 105 F. may be easily borne for a short time, but it becomes alarming if much prolonged.
The tongue of newborn infants is generally whitish and continues to be so until the saliva becomes plentiful. After this we usually find it coated in disturbances of the stomach and bowels and in nearly any disorder accompanied by fever. In scarlet fever the tongue becomes bright red after a few days, and in measles and whooping cough it is often faintly bluish. In the latter affection an ulcer may sometimes be found directly under the tongue, where the thin membrane binds it to the floor of the mouth. In thrush the tongue is covered with white patches like curdled milk. A pale, flabby tongue, marked by the teeth at its edges, indicates debility or impaired digestion. In prolonged or very high fever the tongue grows dry, and in some diseases of the stomach or bowels it may look like raw beef.258
Grinding of the teeth is a frequent symptom in infants in whom dentition has commenced. It generally indicates an irritated nervous system. Most often this depends upon some disturbance of digestion; less often upon the presence of worms. The symptom is present during or preceding a convulsion, and may occur, too, in disease of the brain. In some babies it appears to be only a nervous habit.
The manner of nursing or swallowing frequently affords important information. A baby whose nose is much obstructed or who has pneumonia can nurse but for a moment, and then has to let the nipple go in order to breathe more satisfactorily. If it gives a few sucks and then drops the nipple with a cry, we must suspect that the mouth is sore and that nursing is painful. If it swallows with a gurgling noise, often stops to cough, and does as little nursing as possible, we suspect that the throat may be sore. The ceasing to nurse at all, in the case of a very sick baby, is an evidence of great weakness or increasing stupor, and is a most unfavorable symptom.
Urine that is high-colored and stains the diaper, or that shows a thick, reddish cloud after standing, may accompany fever or indigestion. Sometimes the urine under these conditions is milky when first passed. In some babies a diet containing beef juice or other highly nitrogenous food will produce the reddish cloud, or even actual, red, sandlike particles. A decidedly yellow stain on the diaper occurs when there is jaundice. A faint reddish stain seldom indicates blood. The amount of urine passed is scanty in fever, in diarrhea, and especially in acute Bright's disease. In the latter disease the urine is often of a smoky or even a muddy appearance. The possibility of the occurrence of this symptom after scarlet fever must always be kept in mind, in order that a physician may be summoned very quickly, since it is a serious matter.
We find that the passages are often putty-colored in disorders of the liver, frequently bloody or tarry in appearance in bleeding within the bowel, and liable to be black after taking bismuth, charcoal, or iron, and red after krameria, kino, or haematoxylon. Infants who are receiving more milk than they can digest constantly have whitish lumps in their stools, or even entirely formed but almost white259 passages. The presence of a certain amount of greenish coloration of the passages is not infrequent. This is usually an evidence of indigestion, but passages which are yellow when passed and turn to a faint pea green some time later are not an indication of disease.
3 From Griffith's Care of the Baby, copyrighted by W. B. Saunders Company.
When baby shows that he is sick, take his temperature as directed elsewhere, cut down the feeding to at least one half, or, if his temperature is around 102 F. give him nothing but rice water or barley water. If he is constipated give him a cleansing enema, and if hot and feverish a sponge bath may be administered. He should then be put into a bed with light covers and wait further orders which the doctor will give on his arrival. Give the baby no medicine unless ordered to do so by the physician.
Known to every physician who undertakes the care of children, is the failure of many well-meaning mothers to call him early. The mother attempts the care of the baby herself, and not until the condition gets beyond her knowledge and wisdom does she seek medical advice. In the early hours of an approaching cold, the beginning of intestinal indigestion, or at the beginning of bronchitis, if the physician can see the child early, prolonged illness may be avoided as well as unnecessary expense and many heart-breaking experiences.
Feeding the sick baby differs somewhat with the character of the individual disease, but in the outset of any and all diseases the intestinal tract should not be overburdened with food. At the approach of any illness, the food should at least be cut down one half; for instance, in the case of a serious acute illness accompanied by fever, not only should the strength of the food be reduced one half, but water should be given plentifully between feedings. It is better never to urge the baby to eat at such times—for the ability to digest food is very much reduced.
In cases of acute attacks with much vomiting and fever, all milk should be immediately stopped and rice water or bar260ley water substituted. When vomiting ceases and the fever approaches normal and food is desired, begin with boiled skim milk in small amounts, well diluted with cereal water, and do not approach the normal amount of milk for twenty-four to forty-eight hours. In this way the weak digestive organs are not overtaxed and they gradually resume their usual work of good digestion. When a baby seems to have no appetite for food, lengthen the intervals from three to four or five hours, for feeding when food is not desired usually aggravates disease disturbances.
And now, above all times, the early seed sowing of teaching the child self-control, teaching him to gargle if he is sufficiently old enough, to open his mouth and allow observation without resistance, brings sure results. The great harm of making the doctor and his medicine a threat to obtain obedience also brings its harvest at this time; for the doctor, of all people, ought to be regarded as the child's best friend. When baby is sick, the doctor is needed, his daily visits must not be resisted, his medicines must not be feared—these and such other matters should be made a part of every child's early education.
Under no circumstances or conditions should we directly falsify to a child. Nothing is accomplished by telling a child it will not hurt when you know that it will hurt, or that the medicine tastes good when you know it is bad-tasting. Every physician can recall unnecessary disturbances in the office because a mother has allowed a child to acquire a wrong mental attitude toward the family physician.
One mother told her little girl in my office when I wished to make an examination for adenoids which necessitated my putting my finger back of the child's uvula, "Now Mary, the doctor won't hurt you at all, it will feel nice." I turned to the little girl and said: "Mary, it will not feel nice, it really won't hurt you, but it will feel uncomfortable." It was a grave mistake to tell her that it would feel nice. The child resisted, and, while the examination was successfully made, the greatest of261 tact had to be used in securing the friendship of the child after the examination.
It is far better when the throat is to be examined to wrap the child in a shawl or a sheet with his arms placed at his side, and for a member of the family to take him in her lap and hold him securely while the physician quickly makes the observation. And while we appreciate that sickness is not the time to introduce new methods of training, in instances where children have been spoiled, it is far better quietly and firmly to go about the task in a manner that you know can be carried through to a successful finish.
A sick child should be encouraged to lie in his bed much of the time, and the bed should be kept clean and cool. He should never be set up suddenly or laid back quickly. In the case of a broken leg, all rapid movements should be avoided. A simple story or a soothing lullaby, or the giving of a toy, will often divert attention when some painful movement must be made or some disagreeable task performed.
Both cleanliness of the body and cleanliness of the mouth are exceedingly necessary in sickness. In all instances of disease or indisposition, the mouth must receive daily care, for stomatitis or gangrene of the mouth often follows neglect. A listerine wash in proportion of one to four, or a magnesia wash, or the addition of a few drops of essence of cinnamon to the mouth wash will do much to prevent such conditions, as well as to relieve them.
Applications of medicine to the throat may be made without resistance if the tactful nurse watches her time. She should slowly introduce the tongue depressor which may be a flat stick or a spoon, when the application of medicine with a camel's-hair brush is quickly made to the rolled-out throat as the child gags, and if the nurse then quickly diverts his attention to some beautiful story or a picture or a new toy, the treatment is soon forgotten. Under no circumstances argue with or scold a sick child. Get everything ready, if possible behind his back or in another room, and then with plenty of help make the262 application or the observation without words, always with gentleness and firmness.
Whether the nurse be the mother, caretaker, practical or professional nurse, a record should always be kept of the condition of the patient. The temperature should be reported at different periods designated by the physician. The pulse should be recorded, the amount of urine passed and the time it was passed, the number of bowel movements, all feedings and the general well being of the child—whether it is restless or comfortable, sleeping or awake, together with the water that he drinks.
The record may be kept, if necessary, on a piece of common letter paper, and should read something like this:
March 26, 1916
7 a. m. Temperature 102; pulse 132; respiration 40; morning toilet; took 4 ounces of milk; 2 ounces of barley water; 1 ounce of lime water.
9 a. m. Enema given; good bowel movement; mustard paste applied to chest, front and back, and oil-silk jacket applied; drank boiled water, 4 ounces.
11 a. m. Took the juice of one orange; temperature 103; pulse 135.
12 Noon. Very listless and nervous; temperature 104. Has coughed a great deal. Gave mustard paste to chest, front and back, and wet-sheet pack.
1:30 p. m. Temperature 101.8; 4 ounces of water to drink; looks better.
3 p. m. Has slept 1-1/2 hours; temperature 102.5; pulse 134; respiration 40; 6 ounces of food given (3 ounces of milk, 2 ounces of barley water and 1 ounce of lime water).
A record like this is a great help to the physician, and such a record may be kept by anyone who can read and write. There are printed record blanks which may be procured from any medical supply house and most drug stores.263
Castor oil has neither a pleasant smell nor taste, and nothing is accomplished by telling the child that it does smell good or taste good. If the patient is old enough to drink from a cup, put in a layer of orange juice and then the castor oil and then another layer of orange juice, and in this way it often can be easily taken. Someone has suggested that a piece of ice held in the mouth just before the medicine is taken will often make a bad dose go down without so much forcing. A taste of currant jelly, or a bit of sweet chocolate, or the chewing of a stick of cinnamon is a great adjunct to the administration of bad-tasting medicines. All oily medicines must be kept in a cool place and should always be given in spoons or from medicine glasses that have first been dipped in very cold water. Very often the addition of sugar to bad-tasting medicines will in no wise interfere with their action, while it often facilitates the administration of the disagreeable dose. The majority of bad-tasting medicines are now put up in the form of chocolate-flavored candy tablets.
The normal temperature of a baby is 98.5 to 99 F. in the rectum. After shaking the mercury of the thermometer down below the 97 mark it is well lubricated with vaseline and then carefully, gently, pushed into the rectum for about an inch and a half or two inches, and left there for three minutes before removing.
Mothers should exercise self-control in taking the temperature, for nothing is gained by allowing a panicky fear to seize you should the mercury register higher than you anticipated. Notify your physician when the temperature registers above 100 F.
The respirations of a child are fairly regular and rhythmic and occur about forty times per minute during the first month of life and about thirty times per minute during the remainder of the year. From one to two years, twenty-six to twenty-eight is the average. Breathing is somewhat irregular when264 the child is awake and may be a bit slower when asleep. Before the baby is born the fetal pulse is about 150. At birth it ranges from 130 to 140. During the first month the pulse is found to be from 120 to 140. By the sixth month it gets down to 120 or 130, and from that on to a year the normal pulse beat of the baby is about 120. The pulse is influenced very much by exercise and is often increased by crying or nursing or any other excitement.
Children get fever very easily—the digestive disturbance of overeating, constipation, a slight bilious attack—all produce fever which disappears quite as suddenly as it came. The first thing to do under such circumstances is to withhold food, give plenty of water to drink, produce a brisk movement of the bowel by giving a dose of castor oil, give a cleansing enema, and treat the fever as follows:
After removing all of the clothes from the child, place him in a warm blanket and then prepare a sponge bath which may be equal parts of alcohol and water; expose one portion of the body at a time and apply the water and alcohol first to one arm and then to the other arm, the chest, one leg, the other leg, the back and then the buttocks. Do not dry the part but allow evaporation to take place, and this, accompanied by the cooling of the blood which is brought to the skin by the friction, readily reduces the fever. Another procedure which may be employed if the fever registers high is the wet-sheet pack which is administered as follows:
Three thicknesses of wool blankets are placed on the bed and a sheet as long as the baby and just enough to wrap around him once, is wrung out of cool water and spread over these blankets. With a hot-water bottle to the feet, the child is then laid down in the wet sheet which is now brought in contact with every portion of his body, then the blankets are quickly brought around, and he is allowed to warm up the sheet—which lowers his temperature.
Another valuable procedure is the cooling enema. Water the same temperature as that of the body, is allowed to enter265 the bowel and is then quickly cooled down to 90 or 85 F.; in this manner much heat is taken out of the body and the fever quickly reduced. (For further treatment of fevers see Appendix.)
Visitors should never be allowed in the sick room during the height of a disease, and during convalescence not more than one visitor should be allowed at one time, and the visit then should be only two or three minutes in length. The order and the quietness and the system of the sick room should be perfect. Visitors and loitering members of the family do no good and they may do much harm to the recuperating nervous system of the child.
In these days of high rents, we realize that the greater per cent of our readers are living in apartments and homes just big enough conveniently to care for the family during health, and while it would be pleasant and convenient to have a spare room or an attic chamber that could be used in case of illness, it is the exception rather than the rule that the families to whom sickness comes have these extra apartments. When a contagious or an infectious disease comes to the family, it is of great importance that the sick child be isolated, preferably on another floor, from that used by the immediate family.
Those living in homes, more than likely can fix up a room on the attic floor for the isolation, and those living in apartments may put the sick child in one end of the apartment, while they inhabit the other end. One family under my observation not long ago had a child stricken with the measles. In the same apartment there lived a puny baby not quite two years old. Coming as it did in February, the mother of the child was apprehensive, fearing that measles would leave a severe bronchitis which might mean the death of the already too-delicate267 baby. She was instructed to move the baby's bed to the sun parlor in the front of the flat, while the boy with the measles was put in the parents' room in the rear end of the flat. A sheet was suspended in the middle of the hall leading from the living-room to the bedrooms. Door knobs were disinfected daily, a caretaker was put in charge of the measles patient, the mother very frequently was compelled to go back and administer a treatment, but each time she donned a large apron and completely covered her hair with a towel, she administered the treatment, took off her wrappings, thoroughly washed her face and hands—disinfected them—and returned to her baby in the front part of the house.
At night this mother slept on the floor on springs and mattress in the living-room, and to that home the measles came and departed, and the baby did not get them at all, so perfect was the isolation, so vigilant the disinfection, and so scrupulous the care to prevent contamination. So you see from this one instance that it is altogether possible to make isolation complete even on the same floor. But, mind you, the dishes that the lad ate from were all kept in his room. Food was brought to the sheet and there the caretaker held her dishes while the cook poured or lifted the food from her clean dishes to the dishes the caretaker brought from the sick room.
Whether the sick room is in the attic or whether it be the rear end of an apartment, if the principles of contagion and disinfection are understood I believe it is perfectly possible to isolate even scarlet fever without danger to the other members of the family.
For slight indispositions and trifling disorders, it is not necessary to strip the room of its adornment, but it is well to clear off the dresser tops, protect them well with many thicknesses of newspapers covered over by a folded sheet so that alcohol, witch-hazel and other necessaries will not injure the mahogany or oak-top dresser. Whenever the children are sick, rob the room of anything that is going to be in your way. In instances of infectious or contagious diseases, take down all silk or wool268 hangings, replace them by washable curtains or inexpensive ones that can be burned if necessary, and remove valuable paintings and other bric-a-brac that later fumigation will harm or that may gather the dust during the days of illness.
Just as it is necessary for the man who mines the coal to wear suitable garments, and for the woman who does the scrubbing to dress accordingly, and for the nurse who cares for the case to wear washable clothes—so it is necessary to dress the sick room in garments that are suitable, convenient, and capable of being thoroughly disinfected, fumigated, or even burned if the occasion demands. Hence, expensive rugs should be replaced by rag carpets or no rug at all, while unnecessary articles and garments should be removed from closets, etc.
Remembering that the little fellow is to remain in this room for possibly two weeks or maybe six weeks, let us put up some bright-colored pictures that he will enjoy, bring in some books and magazines by which he may be entertained, secure a few simple toys that will not tax the brain, but serve as a help to pass away the long hours. There are many paper games that may be had, such as transfer pictures, picture puzzles, kindergarten papers, drawing pictures, as well as toys that may be put together to fashion new articles. A whole lot of fun can be gotten out of a bunch of burrs that can be stuck together to make men, animals, houses, etc. Scissors and pictures are entertaining as well as paper dolls with their wardrobes. Rubber balloons, or a target gun for the boy of six will be a great source of delight to him; as will a doll with a trunk full of clothes for the little girl during her convalescent days. A tactful nurse and a resourceful mother will think of all the rest that we have not mentioned—which will amuse, entertain and keep happy our convalescent children, help them to forget that they are "shut ins."
It is wise in instances of the more severe childhood troubles, such as infectious and contagious diseases, to keep as many things in the sick room as possible, and so we remind our reader of the home-made ice box, described elsewhere in this269 book, in which may be kept the fruit juices and the fruits, as well as the milk and the buttermilk. Many medicines, particularly the oily medicines, should be kept in this home-made ice box and five cents worth of ice a day will not only make things taste better, especially during the warm months, but will protect the other members of the family, for the family ice box is a big central station which must be protected against infections and carriers of disease.
In connection with the ice box, we are reminded that it would be a great convenience to have a simple contrivance for heating bouillon, milk, or making a piece of toast, which can be readily done with an electric heater, an alcohol stove, or a small apparatus fitting over the gas jet.
The most important thing which we are going to mention in this division of the chapter is the disinfection of the door knobs. According to the directions on the poison bottle, place an antiseptic tablet into a small amount of water which will make a solution of 1 to 1000 of bichlorid of mercury, and several times a day disinfect the door knobs, particularly in the sick end of the house—thoroughly washing and adequately rubbing with a towel moistened in this solution.
All stools and urine from the sick one will receive attention as directed by the physician. The stools from a typhoid patient should stand for one-half hour in a chamber covered with a layer of lime.
It is not at all necessary to have vessels containing disinfectant substances standing about the room and in the closet. In a room adjoining should be kept all of the dishes used by the sick patient, his tray, half a dozen napkins, knife, fork, spoon, serving dishes, drinking glass, pitcher, etc. All bedding and all linen used by the sick member should be allowed to stand in a solution of disinfectant for several hours when they may be wrung out of the solution, dropped into a bucket and carried to the laundry without any danger to other members of the family.
The nurse is not allowed to leave this room in the garments270 that are worn while caring for the sick. She should have her meals in an adjoining room which is also under strict isolation.
The sick room medicine chest should be so placed on the wall that it is outside the reach of the smaller members of the family, for in it should be placed poisons for external use that are capable of producing death if taken internally. Bottles that hold these poisons—such as bichlorid of mercury, lysol, carbolic acid, laudanum, paregoric, belladonna, etc.—should be so different from the other bottles in the medicine chest that if one should reach for them with his eyes shut or in the dark he would at once recognize that he had hold of a poison bottle. This is absolutely necessary. It usually means a bit of extra expense, but when we realize what tragedies may be avoided by such slight expense, it must not be considered.
Bottles may be procured that have been molded with points of glass projecting from the outside which make them rough to the touch, or they may be covered with a wire mesh or with a wicker covering which may easily be told from the other bottles in the case.
One woman lost her life because the nurse placed two ounces of carbolic acid in the enema instead of two ounces of saline solution. Saline solution is nothing but salt and water, while carbolic acid cost the woman her life, simply because the carbolic acid was not placed in a specialized poison bottle and the attendant could not read the label in the dark.
Under no circumstances keep from one year to another the remnants of unused medicine of a former sickness, for medicines do not keep well and often lose their strength if kept longer than the physician intended.
In this medicine chest should be found the following articles:
A glass graduate marked with fluid drachms (1 teaspoon), and fluid ounces (8 teaspoons).
A medicine dropper.
Absorbent cotton.
271Boric acid.
Camphorated oil.
Castor oil.
Aromatic spirits of ammonia.
Alcohol.
Olive oil.
Epsom salts.
Soda-mint tablets.
Vaseline.
Zinc ointment, together with other medicines the physician orders.
Ice bag, hot-water bottle and oiled silk.
Besides these articles, in the nursery—in readiness for emergencies and accidents—should be found the following:
Gauze bandages of various sizes.
Sterile gauze.
Boric acid crystals and powder.
Mustard.
A pocket case of instruments containing scissors, knife, dressing forceps, etc.
Syrup of ipecac.
Glycerin.
Tincture of iodine.
Package of ordinary baking soda.
Peroxid of hydrogen.
Absorbent cotton.
Needle and thread.
Lime water.
Aside from the giving of castor oil and the application of vaseline to the nose, or of applying boracic acid to the eyes, no medicine should be administered to the baby without competent medical advice. There are numerous widely advertised nostrums frequently sold as soothing syrups to be used during the teething or during attacks of diarrhea, or cough spasms, croup, or worms, that contain dangerous drugs and should not272 be given to children. Many well-meaning but ignorant mothers are slowly but surely laying the foundations for serious nervous disorders and are often making veritable dope fiends out of their children. Patent medicines are dangerous things in the hands of the people; if we are going to give medicines to our little babies let us at least know what we are giving. Let some conscientious, scientific physician examine the baby and prescribe for its needs.
If urged to use a patent medicine, examine the label carefully, for the Federal Food and Drug Act requires the manufacturer of patent medicines to print plainly on the label of the bottle the name and amount of certain dangerous drugs which it may contain.
The drugs mentioned in this drug act and which are often used in patent medicine nostrums are, chloral hydrate, cocaine, heroin, chloroform, alpha or beta eucaine, opium, morphin, alcohol, cannabis indica, or any derivative or preparation of any such substance contained therein.
There are many other drugs sold on the market containing syrups or flavoring materials which may do harm—which may upset the baby's digestion.
Mothers avoid patent medicines. Consult your physician. Never give a baby any sort of medicine to induce sleep. Unless babies are sick or spoiled or hungry, they will go to sleep of themselves, and even in the days of a high fever a wet-sheet pack seldom ever fails to put the baby to sleep and can do no harm if properly given.
This may be as good a place as any to mention the dosage of castor oil which is as follows:
Up to three months, ½ teaspoon.
From three to six months, 1 teaspoon.
From six to nine months, 1½ teaspoons.
From nine to twelve months, 1 dessert spoon (2 teaspoons).
From twelve months on, 1 to 2 tablespoons.
The physician will direct when the disinfectant bath is to be given to the patient previous to his liberation from isolation.273 The different diseases demand different treatment, but, on the whole, it is about as follows:
The day before the boy is to be allowed to go out among the family once more he receives a soap wash, clean sheet and bedding on the bed, and puts on clean garments. The following morning, his head thoroughly shampooed, his nails manicured, a second soap wash is given followed by a weak bichlorid bath (1 to 10,000 solution) which is followed by an alcohol rub. He is then allowed to go out of the sick room which is now to be thoroughly disinfected and fumigated.
After the illness is over, the sick room and the adjoining closets and ante rooms must be thoroughly disinfected or fumigated. If you are located in a city, the health authorities will do this after an infectious or contagious disease. Away from such conveniences, use the following method:
Place two ounces of crystals of permanganate of potash in a pan and have a pint bottle of formalin near by. Everything in the room is now exposed, dresser drawers are opened, all bedding, all garments—in fact everything that is in the room—is put in such a position as to be readily exposed to the fumes which are to follow. A line should be stretched across the room over which are thrown the bedding, garments, etc. The cracks of the windows and doors, except the one door of exit, are now sealed up with paper which has been dipped in green soap, and having the paper strips and pan of green soap ready just outside the exit door, the formalin is now poured over the permanganate crystals. Fumes will immediately arise and permeate every corner, crack and crevice of the sick room. Now quickly make your exit, close the door and seal up key hole and cracks and space under the door with paper dipped in green soap. Leave the room for six hours. After this with a well-moistened cloth to the nose, rush in and throw the windows open, hurry out and allow the room to air from twelve to twenty-four hours, after which wash woodwork and painted walls or take paper off and repaper walls; recalcimine ceilings and closets; scrub closet shelves and dresser drawers, bedsteads, and other furniture thoroughly. If the mattress is old throw it away, but if not, sun it for several days following the fumigation.
In this chapter we will consider the diseases which commonly occur during infancy and early childhood relative to digestion and the alimentary tract. Irregularity of feeding, feeding between meals, feeding too much at any given time, as well as feeding the wrong kind of food may cause stomach disturbances and intestinal troubles.
In a previous chapter, "The Feeding Problem," a common stomach disturbance, vomiting, was gone into quite thoroughly, and in passing to other disorders, we wish to remind the mother that vomiting should always be taken seriously. The interval between meals should usually be lengthened, the time spent in feeding shortened, and it is often necessary to withhold all milk and food of any kind for twelve or eighteen hours, giving only boiled, unsweetened water. Vomiting frequently ushers in some acute disease, and in remote cases, when it is very persistent, it may indicate inflammation of the brain. Complete rest is essential, trotting on the knee, suddenly changing the baby's position, or other quick movements must all be avoided. A physician should see the sick one and determine the cause of the trouble.
Cases of ordinary colic are usually relieved by heat to the abdomen and feet, drinking hot water in which there has been dissolved a pinch of ordinary baking soda, or a portion of a soda mint tablet, or by the use of the photophore, as previously described. The treatment of such ordinary colic need275 not be given further consideration here because it has been described at length in a former chapter; but we do call the attention of the mother to a more serious form of recurring colic which so often accompanies chronic intestinal indigestion, marasmus, and malnutrition.
In most instances the food is radically at fault and should be reduced to a mixture which can more readily be digested and assimilated by the child. Often whey mixtures, peptonized foods, or buttermilk may be indicated. The weight of the baby, the age of the baby, and the color of the stools, must all be taken into account in the preparation of this easily digested food. Weak mixtures should be given at first and then gradually and carefully the quality may be strengthened until the normal formula is again used for the baby.
Injections into the bowel of water, to which has been added one level teaspoon of soda to the pint, will often give relief in this form of colic.
While this condition may occur at any time during babyhood days, it often makes its appearance during the last half of the first year and up to the fifth year. It is accompanied by mucus in the stools, chronic flatulence, constipation or diarrhea, or the alternating of the two, restlessness at night, distention of the abdomen ("pot bellied") accompanied by pain, a coated tongue with a fetid breath, and loss of appetite. It is a pitiable picture—the weight is usually reduced and the child gives the appearance of being decidedly undernourished. This condition is usually occasioned by errors in diet, whether it be over-feeding or feeding of the wrong element of food, and, since the diet is usually responsible for the condition, in the line of treatment diet is a prime factor.
All fats must be taken from the food, sugars should be avoided, and the amount of starchy foods, such as flour, potatoes and bread, should be greatly reduced. Buttermilk, skimmed milk, eggs, green vegetables, and fruit juices should be given. In the older child, if grains are used, they should be well toasted or baked.276
It is altogether common and physiological for the newborn baby to pass through a few days of yellow skin which usually clears up in the second or third week, but it should not recur. Occasionally this yellow tint deepens, the whites of the eyes are yellow, the urine passed leaves a yellow stain on the diaper, while passages from the bowels are white or clay colored. If the child shows symptoms of ill health other than the yellow tint, it should receive medical attention. Older children troubled with jaundice should receive the following treatment: The photophore as described elsewhere should be applied to the liver and abdomen (the liver is on the right side), and this should be followed by the application of what is known as a heating compress, consisting of three layers—a cloth wrung from cold water, a mackintosh, and then two thicknesses of blanket flannel—which are all applied when the skin has been made red by the application of heat. (If the photophore is unavailable, a hot-water bottle may be applied.) The flannel is pinned snugly on the outside as the wet cloth goes next to the skin with the mackintosh between. This should remain on the abdomen for three or four hours, after which the hot application is again made to the liver and abdomen. The administration of broken doses of calomel is sometimes indicated in obstinate cases in connection with these applications of heat to the liver. Hot milk or mineral water may be taken with dry toast. In a day or two the color should clear up, the stools should be normal again, and the treatment may be discontinued.
Irritation about the rectum which cannot be otherwise explained is usually suggestive of pinworms. These seatworms or pinworms are very much like little pieces of cotton thread—one-fourth of an inch in length. They grow and thrive in the lower part of the large bowel. Simple and effective treatment is as follows:
It is well to bathe the parts about the rectum after each bowel movement and often two or three times a day with a277 weak antiseptic solution. Itching may be controlled by the application of a disinfectant ointment, or the local applications of ice may serve the same purpose. After a thorough cleansing of the colon by an injection of lukewarm water containing a teaspoon of borax to the pint in order to remove the mucus, Doctor Holt suggests that after the discharge of this borated enema, infusions of quassia are very helpful (See Appendix).
Children suffering from roundworms experience a loss of appetite, varying temperature from above normal to subnormal, with colicky pains in the abdomen on coming to the table and beginning to eat. They are pale and listless, or nervous and irritable.
Roundworms very much resemble earthworms in shape and color. While their home is in the small intestines they often travel to other parts of the body. They have sometimes crawled into the stomach and have been vomited. The only definite symptom of worms is to find the eggs or the worms themselves in the stool. No worm medicine should ever be given by the mouth without being prescribed by a physician. Cases are on record where well-meaning mothers have killed their children by giving an over dose of worm medicine.
Tapeworms sometimes trouble children; their segments are found in the stool, and look like small pieces of tape line. The segments are flat and thin, one-fourth inch to one-half inch in width and three-fourths to one inch in length. They are joined together and often their number is so great the worm is many feet in length. The segments grow smaller and smaller as they approach the neck, the head of the worm being a mere point. As the worm is passing from the child it should never be pulled, as the head is easily broken off, and, on remaining in the bowel, it will grow to a full-sized worm.
Worms come from the eating of half-cooked meats; they enter the stomach as eggs or tiny worms, and pass out into the small intestines, where they begin to grow. They are a common parasite in the human family and should be suspected in all instances where digestive symptoms are masked or do not yield to treatment.278
This disease, once seen only in the southern part of the United States, is leaving its former domains as the migrating population is distributing it more or less widely everywhere. Sandy soil and country districts are infected by a tiny worm which thrives in polluted soil and enters the body through the skin of the feet. It also gets into the body through the drinking water or from the eating of uncooked vegetables, such as are used in salads.
The disease is manifested by "sallow skin, paleness, headache, swollen abdomen and sores on the legs." Little swollen places where the worm enters the skin may be seen on the flesh. The condition yields readily to treatment. If a child is discovered scratching his feet (especially in the southern part of this country), he should be taken at once to a physician.
At the first symptom of a disordered stomach take all food from the baby and give him rice water prepared by throwing a cupful of well-washed rice into a kettle of boiling water and allowing it to continue to boil for a couple of hours. The water which is strained off is rice water, ready for use after it is cooled. This may be given to the child at the meal hour in the place of his regular food. It should be kept in a glass-covered jar in the ice box. A dose of castor oil, according to the age, should be administered before the feed. The bowels should be washed out and boiled water given freely between the meals of rice water. For a day or two (twenty-four to forty-eight hours), the child should be fed only this rice water, or until the temperature returns to normal and he appears very hungry, at which time milk, which has been boiled for five minutes, may be added to the rice water, first in one-half ounce quantities and gradually increased. Each day a little more milk is added until baby is taking his regular food again.
Many a death and many acute attacks of summer complaint are avoided by the quick use of castor oil, and by withholding food and stopping the use of milk as soon as the child becomes ill.279
Thrush is evidenced by fretfulness or crying on attempting to nurse. On examination of the mouth it is found to be hot and very tender and covered with little white specks which, if looked at under the microscope, appear to be a fungus growth. If scratched off, the mucous membrane bleeds easily. Thrush often occurs during a fever or in connection with other diseases, and is often due to neglect and lack of cleanliness about the bottles, nipples, etc. Taken in time it is quickly cured. An immediate dose of castor oil or milk of magnesia is indicated, and the use of a mouth wash which will be prescribed by the physician. If neglected, it may become ulcerous or gangrenous, which is a very serious condition. Everything pertaining to the feeding, as well as the child's toys, hands, etc., must be kept scrupulously clean.
In the chapter, "The Feeding Problem," constipation in bottle-fed babies was discussed. The bowels should move at least once in twenty-four hours. The passages are frequently very hard and leave the body only after a very great effort of straining. This constipation, often continuing until late childhood, should be corrected in the following manner:
In early infancy—as early as the fourth month—prune juice may be given as directed elsewhere, while in later months prune pulp or fig pulp, which has been carefully rubbed through a fine-mesh colander, may be given at meal time. By the time the baby is eleven or twelve months old, strained apple sauce may be given.
We deplore the use of the water enema as a regular daily procedure; in its place we suggest the use of the enema of oil or the introduction into the rectum of a gluten suppository or in obstinate cases a glycerine suppository. Abdominal massage should be daily administered. With a well-oiled hand, begin on the right abdomen and proceed upward to the lower border of the right ribs and across to the left side and down. This should be repeated many times at a regular hour each day. The mother should select an hour for the bowels to move,280 preferably after the forenoon feeding, and if the child is too small to sit upon the toilet chair, a gluten suppository may be placed into the rectum before the forenoon feed and some time during the middle of the day the bowel movement will be found in the napkin.
For the older child, before a certain meal each day, a well-vaselined piece of cotton may be inserted in the rectum; this often produces a bowel movement immediately after the meal. Laxative foods, such as bran, stewed figs, stewed prunes, or a raw apple, should be used faithfully—as repeated medication never corrects the difficulty, but usually prolongs it.
To immediately flush out the bowel, a soapsuds enema or a plain water enema may be allowed to flow into the lower colon, or a glycerine suppository inserted into the rectum will quickly bring a bowel movement. These methods are only of temporary value; a regular habit should be formed, if possible, to bring about a natural, normal bowel movement. When necessary to resort to drugs—such remedies as cascara sagrada, milk of magnesia, or syrup of rhubarb, are satisfactory, as well as our old stand-by—castor oil. Regular habits must be insisted upon, and if the mother pays attention to regularity at stool in early childhood very little trouble will be met later on in adolescence and adult life.
Chronic constipation often produces abnormal conditions about the rectum such as fissures, hemorrhoids, or prolapse, which may be of serious import.
Diarrhea is a symptom of an acute illness, or it may be associated with a chronic condition such as chronic intestinal indigestion, tuberculosis of the bowel, or may occur alternately with constipation in colitis. It is the most dangerous of all symptoms that babies develop, and in spite of all the instruction given to mothers at the present time, in spite of all the welfare stations in large cities, and in spite of all the efforts put forth by the commissioner of health, with his corps of visiting nurses—even yet, more babies die of diarrhea each summer than from any other single cause.281
There are usually just two reasons for diarrhea—uncleanliness and bad milk. During the hot summer days flies multiply greatly and all manner of bacteria and germs grow in warm, moist, shadowy places, so that usually before the milk leaves the dairy farm it is seriously contaminated with disease-producing germs. If the milk is not kept at a temperature of 35 or 40 F. (which is just above the freezing point), these bacteria, particularly the manure germ, grow at such a rate that by the time the milk gets to the infant it is teeming with bacteria, and diarrhea is the sure result.
Another form of diarrhea is cholera infantum, where the stools soon become watery and colorless. The vomiting is almost incessant and there is high fever. Fortunately it is a rare disease, but when once seen it is never forgotten. One beautiful baby weighing nearly thirty pounds was reduced to sixteen within forty-eight hours, and when death came he could hardly be recognized because of the wasting from this most dreaded of infant diseases.
Another form of diarrhea is seen in an acute inflammatory condition of the intestine itself. The stools contain more or less mucus and blood. The bowel movements, which are very frequent, are accompanied by a great deal of pain and straining. This form is often seen in the more severe types of summer dysentery. We wish to impress upon the reader's mind that these diarrheas may all be avoided if the baby's food is clean and free from germs, if the apple or pear is not only washed, but thoroughly scrubbed before paring during the summer months. If all the bottles, nipples, water, toys, etc., are adequately clean, no summer diarrhea, no dysentery, no other infection due to dirt, will attack the baby. Of paramount importance is the pasteurization of milk during the summer months, as mentioned elsewhere.
Simple diarrhea in the older child of two or three years is treated as follows: Take away all solid foods. Give a big dose of castor oil, thoroughly wash out the bowel by warm water containing a level teaspoon of salt and a level teaspoon282 of baking soda to the pint, and put the child to bed in a quiet room. Boil all milk for ten minutes and thicken it with flour that has been browned in the oven; feed this to the child at five-hour intervals. After each bowel movement, no matter how often they come, the colon should be washed out with the salt and soda enema as before mentioned.
Bear in mind that the child is losing liquids, and so, after the bowels have moved, boiled water should be given by mouth, or a cupful of water can often be retained if it is introduced into the rectum slowly under very low pressure. Twenty-four or forty hours should clear up a case of simple diarrhea, and on returning to food it should be dry toast and boiled milk. For the younger baby, withhold all milk and give barley water or rice water for the first twenty-four hours, returning to milk very gradually and slowly.
For the more severe types, such as the dysentery containing mucus and blood, everything that has been done for the simple diarrhea should be done; the baby should be kept very quiet, while castor oil should be promptly administered. Food is withheld and the bowels are carefully irrigated after each movement with the salt and soda solutions. After the bowels have moved from the castor oil, then bismuth subnitrate, which has been dissolved in two ounces of water, should be given—one or two teaspoons every three hours. This will naturally turn the bowel movements dark.
Under no circumstances should any other medicines be given without the physician's knowledge, as it is at such times as this that many "would-be friends" advise laudanum, paregoric, and other opiates. The skin must be kept warm, and fluids must replace those that have been carried off in the many stools. Water may be given by an enema, by water drinking, and in such rare cases as cholera infantum, when water cannot be retained on the stomach, it often becomes necessary to inject it under the skin (hypodermoclysis) so that it may go at once to the wasted tissues and perhaps save the baby's life.
Give the baby ten days or two weeks to return to normal condition, and under no circumstances hurry the feeding of283 milk, as a second attack may occur much more readily than the first; may more profoundly overcome the baby and result in death.
A protrusion of a loop or portion of intestine through a weakened abdominal muscle—which grows larger when baby cries and smaller when he is lying down in a relaxed condition—is known as rupture or hernia, and is of common occurrence in infancy. It is often seen at the navel and sometimes in the groin as early as the second week.
Hernia is always dangerous and should never be neglected. The physician will protect the navel by a special support with adhesive plaster which is carefully renewed twice a week, and if worn for several months usually entirely corrects the condition. A comfortable truss made from skeins of white yarn will amply protect a groin hernia. The condition should always be taken seriously and receive immediate treatment.
Occasionally, as the result of severe straining in constipation, the rectum protrudes sometimes one-half inch, and in rare instances two or three inches. The placing of a young child upon a toilet chair and insisting upon severe straining sometimes results in such a protrusion of the rectum. This may be avoided by the application of vaseline to the rectum or by the use of the gluten or glycerine suppositories which cause the hardened masses to make their way out easily. Someone has suggested that if the buttocks are supported by a board placed over the toilet seat with a two-inch opening so that severe straining of the rectal muscles is impossible, the prolapse of the rectum will not recur.
The moment the mother observes the slightest protrusion of the rectum she should quickly put it back and have the child lie down and move the bowel in the diaper. Very severe cases require a physician's attention, but if prompt and quick measures are taken on the first appearance it may be quickly corrected and serious consequences be avoided.284
In this connection we might mention a condition which sometimes babies are born with—the absence of the rectal opening. If the baby's bowels do not move for the first two days, surgical interference is more than likely necessary. Often the external opening alone is missing. Sometimes there is a complete closure or atresia of the lower part of the colon.
There should be no hemorrhage from the umbilical stump after it has been properly tied, but occasionally a bit of blood is found upon the dressing and a second tying of the cord stump is necessary. The cord drops off in eight or ten days, and the umbilicus that is left may be moist or it may bleed slightly; if such is the case, great care should be exercised in bathing this ulcer that has been left behind. It simply should be touched with alcohol, a bit of boric acid powder applied, and a small piece of sterile gauze be placed over it. In the course of two or three days it will entirely heal. Care should always be exercised in washing the umbilicus. Extensive hemorrhage from this portion of the body is rare, but it does happen occasionally and is a severe condition which demands surgical attention.
If the umbilicus remains moist and foul smelling, general blood poisoning of the infant may easily follow. Thorough dusting with boric acid powder, with possibly a little oxide of zinc, will usually effect a cure promptly, but should the condition continue, which it does only in rare instances, the doctor may have to cauterize it.
Never under any circumstances knowingly expose a child to any of the so-called "childhood diseases." The old method of "have the child get them as quickly as possible and get over them," has laid the foundation for many chronic disorders later in life. For instance, eye troubles and running ears are often the sequelae of measles; chronic coughs, tuberculosis and bronchitis frequently follow in the wake of whooping cough; heart disorders follow diphtheria, while kidney disease often follows in the course of scarlet fever.
Under all circumstances keep the children away from these dangerous childhood diseases. When a contagious disease breaks out in a school and the little fellow has, along with the other pupils, been exposed to it, begin at once systematically to keep the nose and throat very clean with such well-known sprays as the champhor-menthol-albolene spray, which should be used in the nose morning, noon, and night. Throat gargles, such as listerine, or equal parts of alcohol and water, help to keep the throat in condition to resist the microbic invasion.
During this anxious time of patient waiting the bowels should move every day and the food should be cut down at least a third. In other words, moderate eating and a clean bowel tract go a long way toward keeping a child well and preparing him for an attack of disease. The skin at this time should be kept well bathed and free from the accumulated skin secretions which clog up the sweat glands and otherwise lower the vitality.
Stuffy, close rooms, where the ventilation is poor, not only286 harbor disease germs, but also lower the vitality of the child. Never take your child into a household where there is any form of sickness, for it may turn out to be a contagious disease—no matter how it began, it must be remembered that many contagious diseases, in their earlier stages, much resemble a simple cold.
Measles come on rather gradually, and one might suspect that the child was simply suffering from a severe cold in the head.
Scarlet fever usually begins with a sore throat, while chickenpox has very few initial symptoms; usually the first thing noted is the rash itself. Diphtheria begins with a sore throat, while whooping cough begins very insidiously.
The most important thing is to keep children away from people who are sick, and if a contagious or infectious disease is prevalent in the neighborhood discourage the mingling of the children in hot, illy ventilated rooms. Put a stop to "parties" and all similar gatherings. Let the little folks have good books, plenty of toys, in a well-ventilated room, and the more they keep to themselves at this particular time the better they are off.
It is possible to "stamp out" any known disease if only proper cooperation takes place and certain sanitary regulations are maintained. It is within the memory of most of our readers when yellow fever was put to flight and the cause of malaria discovered. We learned to screen our camps and no longer did our soldiers contract the fever; while the simple covering of stagnant pools with oil, together with proper screenage, stopped the ravages of malaria.
Likewise, many of the woeful tragedies of infant summer diarrhea and dysenteries have been tracked to the so-called "innocent house fly." We have all learned—only recently—that if we move the manure pile once in seven days the hatching of the maggots may be prevented, and so millions, yes trillions, of these carriers of disease may never be born.
If there is one sweet morsel above another for this fly pest287 it is tubercular sputum or feces, and from these feasts they go directly to walk over baby's hands, crawl over his cheek, and wash their feet in his milk. Proper screenage will prevent such contamination of food, such opportunities for carrying disease.
Sunshine, hot water, soap, and fresh air, are the best ordinary every-day disinfectants. It is possible so to conduct the treatment of a contagious or infectious disease that no other member of the family may contract it. A few simple but very important hints are:
1. Door knobs are one of the very greatest avenues of contagion—disinfect them.
2. Cleanse the hands both before and after attending to the sick; first, scrub with stiff brush, soap and water, then dip in alcohol.
3. An epidemic of sore eyes may be stopped by absolute "hand disinfection" and using separate towels.
4. Do not go visiting when you have a "common cold."
5. Kissing is one of the best ways of spreading many diseases.
6. In cases of contagious and infectious diseases completely cover all excretions from the body with lime.
7. Country homes would be as healthy as city homes if the privies and stables were screened.
8. In the country, the well water should be boiled; one infected well may be the cause of the death of a score of beautiful children.
The incubation period of scarlet fever is from one to seven days.
Measles, ten to twenty days.
Whooping cough, from one to two weeks.
Chicken-pox, fourteen to sixteen days.
German measles, seven to twenty-one days.
Diphtheria, any time from one to twelve days.
Mumps, from one week to three weeks.
288
Of all the diseases, measles and chicken-pox are probably the most contagious. In scarlet fever and diphtheria, close contact is necessary for exposure, while whooping cough can actually be contracted in the open air, young babies being particularly susceptible.
Typhoid fever is a disease of the small intestine. Typhoid germs accumulate in the little lymph nodes of the small intestines and that is the reason why we often have so many hemorrhages from the bowel—actual ulcerations take place—and if an ulcer is situated in the neighborhood of a blood vessel hemorrhage may result.
Typhoid fever begins rather insidiously with a slight debility and loss of appetite, but if a temperature record is kept the fever will be found to rise from one-half to a degree higher each day. A steady climb in the temperature curve is noted until the end of the first week, when it remains for a week, possibly 103 or 104 F. After one week it begins slowly to decrease and, if all goes well, the early part of the fourth week usually finds the temperature about normal. It is exceedingly important that the child be kept in bed during the entire course of the disease. The bed pan must be used at each bowel movement or urination.
First Week Treatment. During this week the child may feel quite well, but he should be kept in bed and sustaining treatments begun—such as wet-sheet packs and cold frictions to the skin (during which time there should always be external heat to the feet). The diet must be full and nourishing, but all pastries and "knicknacks" should be avoided. Abundance of fresh fruit that has been well washed before paring, eggs, pasteurized milk, baked potatoes, and toasted bread may be taken at regular periods—with an interval of not less than five hours between meals.
The bowels should be opened in the beginning of the disease with a liberal dose of castor oil, after which daily colonic irrigations should be employed. These enemas should be given at least once a day, the temperature being about that of the289 body, with a smaller terminal enema about five degrees cooler at the close of each bowel cleansing.
Second Week Treatment. The normal temperature at this time is no longer 98.6, it is 101.5 F. This fever is essential to the curative and defensive processes of the body; and while we do not care to have the fever fall below 101.5, at the same time nothing is to be gained by allowing the fever to go up much above 102.5 or 103 degrees F. And so, during the second week, while the disease is at its height, we make frequent use of the wet-sheet pack, always remembering that the extremities must be kept warm and never permitting the skin to become blue or mottled while the cold treatment is being administered. Since the real disease is localized in the small intestine, we will now describe a very important treatment for the diseased bowel—and one which is also very useful in combating high temperature.
The Cooling Enema. The temperature of this enema begins one degree higher than that of the body (supposing the body temperature to be 103, the temperature of the enema would start at 104 F.). This is allowed to flow into the colon and out again, under low pressure, without disturbing the patient, by means of a glass tube connection (See Fig. 15). The temperature is quickly brought down to 100, then to 98, then to 90, usually finishing up at 80 or 85 F. The water is allowed to enter the rectum slowly through a soft rubber catheter (not a hard rectal point), and as it comes out it will be noted that the water is very warm, sometimes registering 105, and it is needless to add that if the water goes in at 80 and comes out at 105 F., much heat has been taken from the body; and so, of all the treatments we have to suggest for typhoid fever, the one just mentioned is possibly the most important. When it is necessary to keep up this enema for an hour or two, the cool water may cramp the bowels, but this may be entirely obviated by applying hot compresses to the abdomen.
Another treatment of great importance in this second week is the cold abdominal compress. Much fever is occasioned in the abdomen because it is the seat of disease, and the much dreaded hemorrhages which often cause the death of the patient are usually avoided by the use of abdominal compresses—wrung out of water at 55 F.—the temperature of ordinary well water—and changed every twenty minutes.
I recall one mother in my dispensary practice who was so poor she could not afford a nurse, her only helper being a son twelve years old. A nurse went to the house twice each day and taught this lad of twelve years to give his mother the cooling colonic irrigation; he was also taught to warm up the abdomen by a hot application and afterwards to apply the cold compresses. The mother made a good recovery.
During this second week the diet should be sustaining. It should consist of boiled milk, eggs, fresh fruit and fresh fruit juices, dextrinized grains (hard toast, toasted corn flakes, shredded wheat biscuits, etc.). The mouth should be kept scrupulously clean, for in all the infectious and contagious diseases there is always the possibility of gangrene in the mouth if it is neglected.
Third Week Treatment. This is the week we look for hemorrhage from the bowel unless the abdomen has been well treated during the second week; and even so, the cool compresses to the abdomen will be continued well into the third week—also the daily or semi-daily enema. The skin is kept in good condition with soap washing and friction baths, and a fairly liberal diet is maintained. During the whole course of the disease the skin is never allowed to get blue or mottled, being quickly restored to the normal red color by the mustard sheet bath, the short hot-blanket pack, or the dry-blanket pack with hot-water bottles. Under no circumstances let the child leave the room or his bed for at least another week.
Infants are rarely affected with mumps. It is a disease of the salivary glands and (as a rule) is usually preceded by pain between the ear and the angle of the jaw, accompanied in a short time by swelling and temperature. It is distinctly contagious even during the incubation period. There is much tenderness on pressure, and chewing is difficult and may be impossible. It usually occurs on the face and only one side may be292 affected. The bowels should be kept open, the mouth should be kept clean, and the side of the face should be protected by a layer of cotton held in place by bandages.
Hot fomentations may be applied if the pain is severe. The electric light bulb on an extension cord, that was mentioned in connection with earache, is very comforting in this condition.
Isolation should be maintained for ten days or two weeks after all symptoms have disappeared.
Scarlet fever is one of childhood's most dreaded diseases because of, first, its long quarantine; second, its terrible possibilities of contagion; and, third, its sequelae.
Absolute quarantine is necessary until ten days after the last signs of desquamation have disappeared.
This disease is always alarming because of the possibilities of its sequelae—the danger of pneumonia, inflammation of the ears, abscesses of the glands of the neck, and nephritis (inflammation of the kidneys).
Scarlet fever is highly contagious at any time during its onset and course. Among the first symptoms of the disease are sore throat, swollen glands, fever, etc. Vomiting on a street car or at the movie may spread the disease to more than one child who might otherwise have escaped. One child who may have only a very light form of the disease may give it to another child in the most severe form. Any such group of classic symptoms—vomiting, fever, rapid pulse, and sore throat—should cause any parent immediately to isolate the little sufferer for several days—awaiting the "rash"—which usually puts in its appearance after three or four days of increasing temperature.
This rash has an appearance "all of its own," unlike any other. Because the fine "meal-like" red points are in such close proximity, the skin assumes a smooth "lobster red" color that is never to be forgotten. After three days of increasing redness, the color begins slowly to fade, and after four or five days of this fading a peculiar peeling takes place, whose293 scales vary in size from a small fleck to casts of the whole of the soles of the feet and the palms of the hands.
During the height of the disease, the throat is very red, the tonsils are not only inflamed, but covered over with white patches, the head aches and the tongue possesses a peculiar coating through which peep the red points of the swollen papillae, presenting the classic "strawberry tongue" of scarlet fever.
After ten days the fever disappears and the "real sick" stage of the disease is in the past.
Each morning of the ten previous days a small dose of Epsom salts is usually administered and the itching, which so often accompanies the rash, is relieved by carbolized-water sponge baths.
The nose, throat, and ears receive daily care—sprays to the nose and gargles to the throat, as well as special swabbing to the tonsils.
The physician in charge of the case will note the urinary findings, guard the heart and kidneys, prevent the spreading of the scales of desquamation by frequent rubbing of the skin with oil, and otherwise work for the future well-being of the patient.
Measles, one of the most common diseases of childhood, is not to be regarded lightly, for very often its sequelae—running ears, weak eyes, and bronchial coughs—may prove very serious and troublesome. Tuberculosis of the lungs not infrequently follows in the wake of measles. The early symptoms of measles are so mild that often the child is out of doors, at school, or about his usual play, until the second or third day of the fever. He was supposed merely to be suffering from a simple "cold in the head."
On the third or fourth day the patient begins heavy sneezing and wears a stupid expression; and it is then that the mother ascertains that his temperature is perhaps 101 to 102 F. He is put to bed and the next day the rash usually appears. The rash is peculiar to itself, not usually mistaken for anything else, being a purplish red, slightly elevated, flattened papule, about294 the size of a split pea. The coughing, which is very annoying, usually remains until about the seventh or eighth day—at which time the fever also disappears.
The bowels must be kept open; a daily bath be given—in which has been dissolved a small amount of bicarbonate of soda (simple baking soda)—after which an oil rub should be administered. The nose should be frequently sprayed with three per cent camphor-menthol-alboline spray, while the throat is gargled with equal parts of alcohol and water. The feet should be kept warm by external heat, while the physician in charge may order additional attention to the chest, such as a pneumonia jacket, etc.
Care should be taken to guard against "catching cold," for bronchitis or pneumonia is quite likely to develop in many cases of measles. The eyes should be protected by goggles and the room should be darkened; under no circumstances should the little patient be allowed to read. Carelessness in this respect may mean weakened eyesight all the rest of his life. Until two weeks after the rash has disappeared, the little fellow should be kept by himself, for the desquamation keeps up almost continuously during this time.
The food during the course of the disease is a liquid and soft diet. Children should never be allowed to go to a party or gathering with a cold in the head; the mothers of a group of small children will never forget the time that one certain mother allowed her little fellow to attend a party with "simply a cold in the head." He laughed, talked, and sneezed during the afternoon and when he went home the rash appeared that night, while eight of the ten exposed children came down with measles during the next two weeks.
The incubation period of chickenpox is from ten to seventeen days. It is a mild disease, with a troublesome rash consisting of widely scattered pimples appearing over the scalp, face, and body. These pimples soon became vesicles (small blisters), which in turn quickly become pustular, afterwards drying up with heavy crust formation. Severe itching which295 attends these pustules may be greatly allayed by either the daily carbolic-acid-water bath or a baking-soda bath. The itching must be relieved by proper measures, for if the crust is removed from the top of the blebs by scratching, a scar usually results. The bowels should be kept open, the diet should be soft. Rigidly isolate, for chickenpox is highly contagious.
This disease occurs oftenest during the cold season. It spares no one unless vaccinated, attacking children and adults alike. The early symptoms are: headache, pain in the back, high fever, vomiting, and general lassitude. In many respects these resemble the symptoms of the grippe, while on the third day the eruption appears. The pimples are hard and feel like shot under the skin. Within a day or two these shotlike pimples have grown and pushed themselves beyond the skin into little conical vesicles which soon turn to pus. By the eighth or ninth day crusts are formed over the vesicle, beginning to fall off about the fifteenth day.
Patients are quarantined usually eight weeks and when a case of smallpox in the home breaks out everyone in the family should be revaccinated. The strictest isolation is important from the first of the disease.
We will not enter into the treatment of smallpox, for medical aid is sought at once and usually the patient is removed to a special isolation hospital.
The history of the change brought about in the Philippines since vaccination has been introduced is an argument of itself which ought to convince the most skeptical of the value of vaccination. By all means, every child in a fair degree of health should be vaccinated. It is wise to vaccinate babies before the teething period—from the third to the sixth month. Babies with any skin trouble or suffering from malnutrition, but not living in a smallpox district, should be vaccinated during the second year. In young babies, under six months, the leg is the proper place to receive the vaccination.296
If proper surgical cleanliness is practiced and ample protection is afforded in after dressing, vaccination need not be a taxing process. The child suffers from general lassitude—a little drowsiness with loss of appetite and a small amount of fever—but this passes off in a reasonable length of time, especially if he is not overfed and his bowels are looked after. On the second or third day after vaccination a red papule appears which soon grows larger, and, after five or six days, it becomes filled with a watery fluid. By the tenth day it has the appearance of a pustule about the size of a ten-cent piece, surrounded by a red areola about three inches in diameter. At the end of two weeks the pustule has dried down to a good crust or scab, in another week it falls off, leaving a pitted white scar.
If the vaccination does not take, it should be repeated after an interval of two months.
Diphtheria is a disease much dreaded during childhood and adolescence. It may attack any age—even little babies are susceptible. It begins with a general feeling of heavy, drowsy lassitude with a sore throat. White spots appear on the tonsils which may resemble a simple follicular tonsillitis, while in a short time white patches spread over the throat and tonsils.
It is not at all uncommon for this membrane to attack the nose, producing a bloody, pustular discharge; and when it does attack the nose, it is none the less contagious and must be regarded just as seriously. A physician is called at once, and, not only to the child, but to the other members of the family, antitoxin is immediately administered. The disease runs a regular course and its most dangerous complication is the membrane which forms in the larynx and threatens to suffocate the child unless prompt intubation is performed—the slipping of a silver tube in the larynx to prevent suffocation and death. The early use of antitoxin greatly lessens all these serious complications.
Care must be exercised to prevent sudden heart failure; and this is done by raising the child to an upright position with the utmost care; while you insist upon him lying quietly upon his back or his side, long after the disease has left his throat. While297 the throat or nose is the seat of disease, the toxins from these most dreaded diphtheritic microbes spread through the lymph channels and the blood vessels to the heart itself—so weakening that organ that it sometimes suddenly fails, or becomes more or less crippled for life. These serious results are to be prevented by the science of good nursing and the prompt use of antitoxin. In these days the "Schick test" may be administered for the purpose of ascertaining whether one is susceptible to contracting diphtheria.
A physician is always in charge of diphtheria, and he will supply directions for the bowels, the diet, and the sprays for the nose and throat, and the general well-being of the suffering child. Isolation and quarantine should continue for two weeks, and in bad cases three weeks, after the membrane has disappeared from the throat.
A child suffering from a continuous cough, particularly if it is accompanied by a whoop or a condition which is so often seen in children who cough—not able to stop—should not be taken to church, nor to the movies, nor allowed to go to school; neither should he be allowed to leave his own yard. The average duration of the disease is usually six weeks. The child should have an abundance of fresh air, should spend much of his time out of doors, and while in the house should avoid dust of every kind; at night he should not be exposed to drafts. Call the physician early in the case and he may attempt to thwart the progress of the disease by certain administrations of vaccine medication.
In very bad cases, where a young child cannot catch his breath and gets blue in the face—which, fortunately, is uncommon—he should be slapped in the face with a towel wet in cold water; or, he may be lifted into a tub of warm water, then quickly in cold water, then back into the warm, etc. Hygienic measures should prevail, such as keeping the bowels open, the skin clean, and the use of the usual throat gargles and nasal sprays. Do not be misguided by the old-time thought that whooping cough must run its course; for, if medical aid is promptly secured, the298 disease may often be cut short and the severe paroxysms greatly lessened.
Not long ago while in North Dakota near Canada, we took a trip one day just over the border to visit several villages of Russian peasants. We found the boys and girls of nearly the entire village suffering from trachoma—a dangerous, infectious disease of the eyes which spreads alarmingly from one child to another.
We saw the disease in all of its varying degrees among the children. Some of them had swollen, reddened lids. A discharge of pus was coming from the eyes of others, and they could not look toward a light or the sun. This disease is spread in a hundred different ways—through the common use of wash basins, towels, handkerchiefs, tools, toys, door knobs, gates, etc., and that is the reason why these isolated villages of foreign people who could neither read nor write the English language were nearly all so sorely afflicted.
The ordinary condition of "catching cold in the eye" ("pink eye") is just as infectious as the trachoma which we have mentioned, although it is more of an acute disorder and nothing like so serious.
In all such cases a physician is to be called immediately, isolate the patient, and give strict attention to carrying out the doctor's orders.
Another form of inflammation of the eye which was mentioned in a previous chapter, is the inflammation of the eye of the newborn.
In most civilized districts at the present, especially where the cases are attended by a physician, the eyes of all newborn babies are treated with either argyrol or silver nitrate. Just as soon as defective sight is discovered in the child the eyes should be examined at once and proper glasses fitted. While the glimmer and shimmer of moving pictures may seriously interfere with the child's vision, on the other hand, this very thing often discovers the defect in the eyesight earlier than it would otherwise be found out.299
Inflammation of the ears was fully covered in our discussion of adenoids and tonsils, but we would like to add at this time that under no circumstances should a running ear be regarded lightly. A chronic mastoiditis (inflammation of the middle ear) often follows measles, scarlet fever, adenoid infection, and inflammation of the tonsils. The attention of a specialist should be called to it and his instructions most carefully carried out; for, when we have a sudden stopping of the discharge from the ear with high fever and pain behind the ear, sometimes an operation is imperative or the child may be lost.
Next to digestive disturbances, babies suffer more frequently from respiratory disorders—colds, bronchitis, and pneumonia. In fact, during very early infancy, pneumonia heads the list of infant deaths, only to be displaced a few months later by that most dreaded summer disease—diarrhea.
Little tiny babies are so helpless—they are so dependent upon their seniors for life itself—that our responsibility is indeed great. We should put forth our best endeavor to avoid and prevent common colds. Among all the common maladies that afflict the human race "colds" probably head the list; and, in the case of babies and the younger children, the common colds often go on into coughs, croup, bronchitis, and even pneumonia.
Babies should not be allowed to sit or play on cold, drafty floors. They may play on mother's bed whose open side is protected with high-back chairs, or they may play in their own bed whose raised sides are sheltered by blankets.
It is possible for a mother so to disinfect her hands, and so garb herself with clean, washable garments, that, although she may be suffering from an acute cold, she may continue to care for her baby and the baby need not contract the cold.
This most annoying ailment, a cold in the head, is particularly hard on babies because the obstruction of the nasal passages not only makes breathing difficult, but renders nursing well-nigh impossible.
The throat end of the eustachium tube (the ear tube) is found in the upper and back part of the throat, just behind the nose. The infection of the cold extends from both the nose and throat and there results a spreading inflammatory process on through these ear tubes into the middle ear itself. Now if this tube swells so much that it entirely closes, as so often happens in cases of "cold in the head" as well as in constant irritation from adenoids, then may follow a vast train of difficulties—earache, mastoiditis, etc.—with the result that the tiny bones in the middle ear which vibrate so exquisitely may become ankylosed (stiffened) and deafness often follow. Everything known must be done to prevent baby's catching "cold in the head." If the sinuses become infected it may also lead to serious consequences.
When the nose becomes clogged it may be opened up by repeatedly disinfecting the inside of the nose with oily sprays such as simple albolene or camphorated-albolene spray.
The bowels should be quickly opened by castor oil, and the feedings should be cut down at least two-thirds or one-half.
Public drinking cups should always be avoided and kissing the baby be tabooed.302
The treatment of influenza in infancy and childhood is to avoid contact with an older person suffering with the grippe. Ordinarily, the so-called "grippe" is a common, mixed infection—not true influenza. Coryza and cough are the chief respiratory symptoms which attend these widespread epidemics. Often vomiting and diarrhea are seen in the young sufferers.
In cases of grippe put the child to bed and call the doctor. In the case of the older children, the treatment and care to be recommended has been fully outlined by the author in the little work entitled The Cause and Cure of Colds.
Complications from the grippe are very frequent in children—such as severe diarrhea, enlarged glands of the neck, running ears, bronchitis, pneumonia, and sometimes tuberculosis.
Every effort should be put forth to isolate and quarantine the first member of the family to be stricken with grippe so that the remaining members may, if possible, escape an uncomfortable and unhappy siege.
The danger of permanent deafness which so often follows a sore throat as well as a cold in the head, should cause every mother or caretaker earnestly to begin treatment at the very first sign of a sore throat. When a little baby gulps or cries on swallowing, a sore throat should always be suspected and remedial measures promptly instituted.
A most convenient article with which to examine an infant's throat is a small pocket flashlight. The pillars of the throat or the tonsils or both may be much inflamed, and since tonsillitis, diphtheria, and scarlet fever all begin with a sore throat, it is wise early to seek medical counsel in order that the differential diagnosis may be promptly made. We urge the mother, as a rule, not to attempt to diagnose severe cases of sore throat. Send for the physician.
Tonsillitis is a severe form of sore throat which, fortunately, rarely troubles tiny infants; but for every sore throat, while waiting for medical help to arrive, lay your plans to empty the303 bowels, diminish the quantity of the food, swab or spray the throat, and later closely follow the physician's advice concerning the general treatment of the child.
Adenoid growths appear as grape-like lymphoid formations located in the upper and posterior-nasal pharynx. These adenoids secrete a very toxic, thickened fluid, which slowly makes its way down along the back wall of the throat, and reddens and inflames first the anterior and posterior pillars of the throat and then often inflames and enlarges the tonsils.
Adenoids not only obstruct the respiratory passage way to the throat and lungs, but they also exert a harmful influence on the general physical and mental development of the child.
It is nothing less than criminal for heedless parents to allow adenoid growths to remain in the child's post-nasal pharynx. The little fellow's face is disfigured, more or less for life, his mentality dulled, while he is compelled to breathe through his mouth.
An almost miraculous change often follows the complete removal of these obstructive adenoids—the child takes a renewed interest in everything about him. More oxygen finds its way to the tissues, his face takes on better color, he gains in weight, in fact, there appears to be a complete rejuvenation mentally and physically.
The signs or symptoms of adenoids are mouth breathing, restlessness at night, snoring, recurring colds, nasal discharge, swelling of the glands of the neck, poor nutrition, loss of appetite, bed wetting, impaired hearing, lack of attention, and mental dullness. The removal of adenoids is neither a serious or difficult procedure, and they may safely be removed at any age.
Tonsils which remain permanently enlarged and show signs of disease and debilitation—filled crypts—may be removed as early as the fourth or fifth year, if necessary. If proper treatment does not improve the tonsils as the child grows older, their removal should seriously be considered. The tonsils may serve304 some special secretory or defensive function during the first few years of life and we think best, therefore, not to advise their removal—except in extreme cases—until the child is at least four or five years old.
When it is necessary to attack the tonsils, they should be thoroughly dissected out—not merely burned or clipped off. If they are properly removed, the danger of heart trouble, rheumatism, and many other infections may be considered as greatly lessened.
After five years of age the normal tonsils should begin to shrink, and at about the beginning of adolescence they should be no larger than a small lima bean, hidden almost completely out of sight behind the pillars of the throat. While healthy tonsils may serve some useful purpose even in the adult, it is almost universally conceded that the thoroughly bad and diseased tonsil is utterly useless to the body—only an open gateway for the entrance of infection.
A very common disorder of early infancy and childhood is bronchitis—an inflammation of the bronchial tubes—accompanied by severe coughing. Its tendency to pass into pneumonia renders it a disease for skilled hands to treat—a disorder hardly safe for even the well-meaning mother to undertake to manage without medical advice and help. And since bronchitis is usually accompanied by alarming symptoms of high fever, weakened heart, embarrassed breathing, mottled or blue skin, green stools, troublesome cough, disturbed sleep, "stopped up nose," and "choked up throat," it is of utmost importance not only to seek medical aid early, but also that the mother, herself, should have definite ideas concerning the proper manner of doing the following things in the line of treatment:
Mustard Pastes are prepared by mixing one part of mustard and six parts of flour in warm water and applying to the chest between two pieces of thin muslin. It is left on just seven minutes and then talcum powder is thickly sprinkled on the moist, reddened skin; this powder quickly absorbs all the moisture and leaves the skin in a good condition—ready for another paste in three hours if it is so ordered.
The Oil-Silk Jacket, or pneumonia jacket, consists of three layers—the inside of cheesecloth, an inner thin sheet of cotton wadding, and an outside layer of oil silk (procurable at any drug store). It should open on the shoulder and under the arm on the same side. It is worn constantly (change for fresh cheesecloth and cotton every day) during the inflammatory stage; it is removed only during the mustard pastes.
A Steam Tent may be prepared by placing a sheet over the infant's crib and allowing steam to enter from a large paper funnel placed in the nose of a tea kettle of boiling water kept hot on a small stove of some sort.
The mattress and bedding are covered with rubber sheeting and the infant's clothes protected from moisture. The baby should remain in this steamy atmosphere ten minutes at a time.
Another method is to hold baby in arms near the large end of a big funnel placed in a tea kettle on the gas stove or range, and then have an assistant help hold a sheet tent over both the mother and babe. Or the baby carriage may be placed over a small tub of water into which are dropped several hot bricks. A sheet canopy spread over the carriage holds the steam in and baby reaps the benefits of the warm moisture.
Colonic Flushing is necessary when green stools accompany bronchitis. A well-lubricated end of a large Davidson's syringe is inserted into the rectum, and with the hips of the baby brought to the edge of a basin (the heels held in the hands of the assistant), water is forced into the rectum. Not more than one ordinary cup of water should be introduced at any one time. After expulsion, another may be gently injected.
The diet in bronchitis is always reduced so that no extra work will be thrown on the already overtaxed constitution of the child.306
Absolute rest is necessary and perfect quiet should prevail. The humidity of the room should not be lower than 50 at any time, while the air should be moderately cool and fresh.
Numerous other details which may be necessary in the management of bronchitis will be directed by the physicians and nurses in charge of the case.
It is believed that children with enlarged tonsils and adenoids are much more subject to croup than others. Although very sudden in its onset and very alarming, spasmodic croup, fortunately, is seldom dangerous. A little child goes to bed in apparently normal condition and wakes up suddenly with a coarse metallic cough, difficult breathing, and with a distressed expression on the face.
Alternate hot and cold compresses should be applied to the throat—first the hot cloths (wrung from very hot water) being applied over the throat, which should be covered with a single thickness of dry flannel. Then after three minutes of the hot cloths a very cold cloth is applied to the skin itself for one half minute; then more of the hot compress, followed again by the short cold, until five such changes have been made. A bronchitis tent should be quickly improvised so that the child can be "steamed."
Vomiting must be produced by kerosene (three or four drops on sugar), alum and molasses, or ipecac (ten drops every fifteen minutes). Some remedy must be administered continuously until free vomiting occurs. A good dose of castor oil should be given after the spasm. Suitable treatment should be administered through the day to prevent a recurrence of the attack the next night.
The general vital resistance should be raised by outdoor life, improved circulation, good food; adenoids if present, should be removed.
Medical advice should be sought in every case of severe croup, for membraneous croup usually is indicative of diphtheria, and the diagnosis is important, as on it hangs the determination of the administration of antitoxin.307
Pneumonia is always a serious disease. It is accompanied by high fever, painful, very short cough, and rapid breathing with a moving in and out of the edges of the nose as well as the spaces between the ribs. The possibilities of complications are always great—the dangers are many—so that the combined watchfulness of both the mother and a proficient trained nurse are required; not to mention the skill of the physician.
The steam tent, the mustard paste, the oil-silk jacket and the colonic flushing (described earlier in this chapter) may all be asked for by the physician in his untiring efforts to prevent dangerous complications during the course of the disease.
Plenty of moderately cool, fresh air (without drafts) is of great benefit. Never allow blue finger tips, or cold ear tips to exist; send at once for the doctor and administer a hot bath, or wrap in a sheet dipped in hot mustard water while awaiting his arrival. No mother should think of attempting to carry her baby through an attack of bronchitis or pneumonia without the best medical help available.
While each child possesses an individuality all its own, nevertheless, there are certain general principles of psychologic conduct and family discipline which are more or less applicable to all children. The so-called nervous child, in addition to the usual methods of child culture, stands in need of special attention as concerns its early discipline and training. This chapter will, therefore, be devoted to special suggestions with regard to the management and training of those children who are by heredity predisposed to nervousness, over-excitability, and who possess but a minimum of self-control.
The so-called nervous child—all things equal—is the child who is born into the world with an unbalanced or inefficiently controlled nervous system; and while it is all too true that the common nursery methods of "spoiling the child" are often equally to blame with heredity for the production of an erratic disposition and an uncontrolled temper, nevertheless, it is now generally recognized that the foundation of the difficulties of the nervous child reaches back into its immediate and remote ancestral heredity.
I no longer doubt but that many of these babies with a bad nervous heredity, who are born predisposed to Saint Vitus' dance, bad temper, chronic worry, neurasthenia, and hysteria could be spared much of their early troubles and later miseries by prompt and proper methods of early nursery discipline.
These nervous babies are born into the world with an abnormal lack of self-control. Their "inhibition control" over the natural and spontaneous tendency of the nervous system to309 manifest its inherent impulses and passing whims is decidedly deficient. The child is unduly sensitive, whines, hollers, or flies into a violent rage when its will is crossed in the least degree. Such a child sometimes keeps its mother living in constant terror because, when its will is crossed in any particular, it will scream and hold its breath until it turns black in the face and sometimes actually goes into a convulsion.
In dealing with these unfortunate little ones, fathers and mothers, while they should be firm and persistent in their methods of correction, should also be kind and patient; fully recognizing that whatever undesirable traits the little ones manifest they have come by honestly—these naughty tendencies being the result either of heredity or spoiling, for both of which the parents stand responsible.
One of the very first things that a child, especially the nervous child, should learn is that crying and other angerful manifestations accomplish absolutely nothing. The greatest part of the successful training of the nervous child should take place before it is three and one-half years of age. It should early learn to lie quietly in its little bed and be entirely happy without receiving any attention or having any fuss made over it. It should not become the center of a circle of admiring and indulgent family friends and caretakers who will succeed in effectually destroying what little degree of self-control it may be fortunate enough to possess.
When the little one is discovered to be nervous, fretful, impatient, and easily irritated early in the morning, it should be left alone in its bed or in the nursery until it quiets down. If it has a good, healthy crying spell, leave it alone. Let it early get used to living with itself—teach the little fellow to get along with the world as it is—and you will do a great deal toward preventing a host of neurasthenic miseries and a flood of hysterical sorrows later on in life.
You must not expect to train the nervous child by the simple and easy methods which are successful in the case of a normal child; that is, you cannot repeat a simple discipline two or three310 times and have the child learn the lesson. In the case of the high-strung nervous child it requires "line upon line and precept upon precept;" for, whereas a normal child will respond to a certain discipline after it is repeated a half dozen times, the nervous child will require the persistent repetition of such a discipline from twenty-five to one hundred times before the lesson sinks into his consciousness sufficiently to enable him to gain control of his erratic and unbalanced nervous mechanism.
As bad as all spoiling methods are in child culture, they are decidedly disastrous—almost fatal—in the case of the nervous child; and yet it is these delicate, sensitive, cute little things that are the very ones who are most frequently the worst spoiled. Nervous children simply must not be played with all the time. They must be by themselves a great deal, at least this is true in their earlier years.
The nervous baby must early learn absolute respect for authority, so that what it lacks in its own nervous control may be partially made up for by parental suggestion and discipline. Of course, as suggested in a later chapter, the more ideal methods of suggestion, education, and persuasion should be employed in your efforts to secure obedience and promote self-control; but, when through either the deep-rooted incorrigibility of a child, or the inefficiency of the parent's efforts in the employment of suggestion—no matter what the cause of the failure of your ideal methods to control temper, stop crying, or otherwise put down the juvenile rebellion, whether the child has been spoiled on account of company, sickness or through your carelessness—when you cannot effectively and immediately enforce your will any other way, do not hesitate to punish; spank promptly and vigorously and spank repeatedly if necessary to accomplish your purpose. You must not fail in the case of the nervous child to accomplish exactly what you start out to do.
When the little fellow wakes up in the night and cries, see if he needs anything and administer to him. If you have previously tried the method of letting him "cry it out," which is311 usually entirely sufficient in the case of a normal child, and if such treatment does not seem to cure him, then speak to him firmly, give him to understand that he must stop crying, and if he does not, turn him over and administer a good spanking—and repeat if necessary to get results. In dealing with a nervous child we must follow the directions on the bottle of the old-fashioned liniment "rub in until relief is obtained."
No "spoiling practices" should be countenanced in the case of nervous children. They should be taught to sleep undisturbed in a room in the presence of usual noises. They should not be allowed to grow up with a sleeping-room always darkened by day and a light to sleep by at night. They should be taught to sleep on without being disturbed even if someone does enter the room; they should be taught to sleep normally without having to quiet and hush the whole neighborhood.
The early play of nervous children should be carefully supervised and organized. Under no circumstance should they be allowed exclusively to play with children younger than themselves. They must not be allowed to dictate and control their playmates; it is far better that they should play at least a part of the time with older children who will force them to occupy subordinate rôles in their affairs of play; in this way much may be accomplished toward preventing the development of a selfish, headstrong, and intolerant attitude. When the nervous child is miffed or peeved at play and wants to quit because he cannot have his way, see to it that he quickly takes his place back in the ranks of his playfellows, and thus early teach him how to react to defeat and disappointment. The nervous child must not be allowed to grow up with a disposition that will in some later crisis cause him to "get mad and quit."
If the nervous baby has older brothers and sisters, see to it that he does not, through pet and peeve and other manifestations of temper, control the family and thus dictate the trend of all the children's play. Early train him to be manly, to play fair, and when his feelings are hurt or things do not go just to his liking, teach him, in the language of the street, to be "game."312 It is equally important that the little girls be taught in the same way how to take disappointment and defeat without murmur or complaint.
When nervous children grow up, especially if their parents are well to do, and they are not forced to work for a living, they are prone to develop into erratic, neurasthenic, and hysterical women, and worrying, inefficient, and nervous men; and in later years they throng the doctor's offices with both their real and imaginary complaints. These patients always feel that they are different from other people, that something terrible is the matter with them or that something awful is about to happen to them. Their brains constantly swarm with fears and premonitions of disease, disaster, and despair, while their otherwise brilliant intellects are confused and handicapped because of these "spoiled" and "hereditary" nervous disturbances—with the result that both their happiness and usefulness in life is largely destroyed.
The fundamental abnormal characteristic of that great group of nerve-patients who throng the doctor's office is sensitiveness, suggestibility, and lack of self-control. Sensitiveness is nothing more or less than a refined form of selfishness, while lack of self-control is merely the combined end-product of heredity and childhood spoiling. I am a great believer in, and practitioner of, modern methods of psychological child culture, but let me say to the fond parent who has a nervous child, when you have failed to teach the child self-control by suggestive methods, do not hesitate to punish, for of all cases it is doubly true of the nervous child that if you "spare the rod" you are sure to "spoil the child."
Let me urge parents to secure this self-control and enforce this discipline before the child is three or four years of age; correct the child at a time when your purpose can be accomplished without leaving in his subconscious mind so many vivid memories of these personal and, sometimes, more or less brutal physical encounters. Every year you put off winning the disciplinary fight with your offspring, you enormously increase the313 danger and likelihood of alienating his affections and otherwise destroying that beautiful and sympathetic relationship which should always exist between a child and his parents. In other words, the older the child, the less the good you accomplish by discipline and the more the personal resentment toward the parent is aroused on the part of the child.
While it is generally admitted that feeble-mindedness lies at the foundation of most crime, we must also recognize that failure on the part of parents to teach their children self-control is also responsible for many otherwise fairly normal youths falling into crime and intemperance. The parents of a nervous child must recognize that they will in all probability be subject to special danger along these lines as they grow up. The nervous child, as it grows up, is quite likely to be erratic, emotional, indecisive, and otherwise easily influenced by his associates and environment.
Nervous children are more highly suggestible than others, and if they have not been taught to control their appetites and desires, their wants and passions, they are going to form an especially susceptible class of society from which may be recruited high-class criminals, dipsomaniacs, and other unfortunates.
It is true that any spoiled child, however normal its heredity, may turn out bad in these respects if it is not properly trained; but what we are trying to accomplish here is to emphasize to parents that the nervous child is doubly prone to go wrong and suffer much sorrow in after life if he is not early and effectively taught self-control.
If the child of nervous tendencies forms the habit of crying, sulking, or otherwise misbehaving when it is denied its desires, or when something it wants done is not immediately attended to, it will be found an excellent plan simply to stand still and let the little fellow have it out with himself, in the meanwhile kindly reminding him to say, "please mamma," "please papa,"314 etc. I well remember one nervous little girl who would yell at the top of her voice and become black in the face the moment she wanted a door opened or anything else. A few weeks of patience and firmness on the part of the mother entirely cured her of this unbecoming trait.
As a rule, it will be found best not to argue with the nervous child. The moment your commands are not heeded, when you have admonished the child once or twice without effect, take him quickly to the crib or the nursery and there leave him alone, isolated, until he is in a state of mind to manifest a kindly spirit and an obedient disposition. It is an excellent plan quietly and quickly to deprive such children of their pleasures temporarily, in order to produce thoughtfulness; and these methods are often more efficacious than the infliction of varying degrees of pain under the guise of punishment.
Nervous children must be taught to go to sleep by themselves. They are not to be rocked or allowed to hold the hand of the mother or the caretaker. The nervous baby should not be encouraged to exhibit its cuteness for the delectation of the family or the amusement of strangers and visitors. He should be especially trained in early and regular habits, taking particular pains to see that bed wetting and similar bad habits are early overcome; otherwise, he may drag along through early life and become the cause of great embarrassment both to himself and his parents.
The control of these nervous habits is somewhat like the management of the slipping of the wheels of a locomotive when the track is wet and slippery. The little folks ofttimes endeavor to apply the brakes, but they are minus the sand which keeps the wheels from slipping. The parent, with his well-planned discipline, is able to supply this essential element, and thus the child is enabled to gain a sufficient amount of self-control to prevent him making a continuous spectacle of himself.
When nervous children do not walk or talk early, let them alone. Of course, if later on it is discovered that they are manifestly backward children, something must be done about it; but if the nervous child is encouraged to talk too soon there is great danger of his developing into a stutterer or a stammerer.315
Every year we have pass through our hands men and women, especially women, who possess beautiful characters, who have noble intellects, and who have high aims and holy ambitions in life, but whose careers have been well-nigh ruined, almost shattered, because of the hysterical tendency which ever accompanies them, and which, just as soon as the stress and strain of life reaches a certain degree of intensity, unfailingly produces its characteristic breakdown; the patient is seized with confusion, is overcome by feeling, indulges in an emotional sprawl, is flooded with terrible apprehensions and distracting sensations, may even go into a convulsive fit, and, in extreme cases, even become unconscious and rigidly stiff.
Now, in the vast majority of cases, if this nervous patient, when a baby, had been thoroughly disciplined and taught proper self-control before it was four years of age, it would have developed into quite a model little citizen; and while throughout life it would have borne more or less of a hysteria stigma, nevertheless it would have possessed a sufficient amount of self-control to have gotten along with dignity and success; in fact, the possibilities are so tremendous, the situation is so terrible in the case of these nervous babies, that we might almost say that, in the majority of such, success and failure in life will be largely determined by the early and effective application of these methods of preventive discipline.
I was recently consulted by a patient whose nervous system was in a deplorable state, who had lost almost complete mental control of herself, and who really presented a pathetic spectacle as she told of the fears and worries that enthralled her. In an effort to get to the bottom of this patient's heredity I had a conference with her father, and I learned that this woman, in her childhood days, had been constantly humored—allowed to have everything she wanted. She was a delicate and sensitive little thing and the parents could not bear to hear her cry, it made her sick, it gave her convulsions, it produced sleepless nights, it destroyed her appetite, and so she grew up in this pampered way. The father recognized the greatness of his mis316take and he told me with tears in his eyes how, when the ringing of the school bell disturbed his little girl baby, he saw the school directors and had them stop ringing the bell, and he even stopped the ringing of the church bells. He was an influential citizen and could even stop the blowing of the whistles if it disturbed his precious little daughter.
And so this woman has grown up with this nervous system naturally weakened by heredity and further weakened by "spoiling"; and fortunate indeed she will be if off and on the most of her life she is not seeking the advice of a physician in her efforts to gain that self-control which her parents could have so easily put in her possession at the time she was three or four years of age, if they had only spent a few hours then, instead of the many months and years that subsequently have been devoted to medical attention.
We run into many snags when we undertake to discipline the nervous baby. The first is that it will sometimes cry so hard that it will get black in the face and may even have a convulsion; occasionally a small blood vessel may be ruptured on some part of the body, usually the face. When you see the little one approaching this point, turn it over and administer a sound spanking and it will instantly catch its breath. This will not have to be repeated many times until that particular difficulty will be largely under control.
It will be discovered when you undertake to break a bad habit in the case of a spoiled child who is of a nervous temperament, that your discipline interferes with the child's appetite and nutrition. The delicate little creature who has perhaps already given you no end of trouble regarding its feeding, will begin to lose in weight, and even the doctor often becomes so alarmed that he advises against all further methods of discipline. We think this is usually a mistake. Both the nutrition and discipline should be kept in mind and carried harmoniously through to a successful finish. It will be necessary during such troublous times to conserve both the physical and nervous strength of the child; it should not be allowed to run about and over-play, as317 such high strung children often do. It should be given a reasonable amount of physical exercise, and two or three times a day should have short periods of complete isolation in the nursery, where it may quietly play with its blocks and toys, sing and croon or talk as the case may be, but should be left entirely alone.
Wise efforts should be put forth to keep the feeding up to the proper number of calories, and to see, if the child does not gain during this disciplinary struggle, that at least it does not lose; and I give it as my experience that I have yet to see a case in which both the child's nutrition and discipline cannot be efficiently maintained at one and the same time, though it does sometimes require adroit scientific and artistic management. But the game we are playing is worth the effort—the battle must be fought—and it can be fought with the least suffering and sorrowing the earlier the conflict is waged to a successful issue.
I am decidedly opposed to allowing these young nervous children to over-play and thus wear themselves out unduly. This over exhaustion sometimes renders the training of the child much more difficult, as it is a well-known fact that we are all much more irritable and lacking in self-control when we are tired, more especially when we are over-tired and fatigued.
Let me emphasize the importance and value of proper periods of isolation—complete rest and partial physical relaxation. You can take a child who has gotten up wrong in the morning, whose nerves are running away with him, who is irritable, crying at everything that happens, who even rejects the food prepared for him, and who, when spoken to and commanded to stop crying, yells all the louder—I say you can take such a little one back to its crib, place it in the bed and smilingly walk out of the room. After a transient outburst of crying, within a very few minutes you can return to find a perfect little angel, winsome and smiling, happy and satisfied, presenting an entirely different picture from the little culprit so recently incarcerated as a punishment for his unseemly conduct.
But let me repeat that while such methods of discipline often work like magic on normal children, they must be repeated again and again in the case of one who is nervous in order to establish318 new association groups in the brain and to form new habit grooves in his developing nervous system.
There are just two things the nervous child must grow up to respect; one is authority and the other is the rights and privileges of his associates. The nervous child needs early to learn to reach a conclusion and to render a decision—to render a decision without equivocation—to move forward in obedience to that decision without quibbling and without question; that is the thing the nervous man and woman must learn in connection with the later conquest of their own nerves; and a foundation for such a mastery of one's unruly nerves is best laid early in life—by teaching the child prompt and unquestioning obedience to parental commands. At the same time, endeavor so to raise the child that it acquires the faculty of quickly and agreeably adapting itself to its environment, at the same time cheerfully recognizing the rights of its fellows.
It is a crime against the nervous child to allow it to hesitate, to debate, or to falter about any matter that pertains to the execution of parental commands. Let your rule be—speak once, then spank. Never for a moment countenance anything resembling dilatoriness or procrastination, let the child grow up to recognize these as its greatest dangers, never to be tolerated for one moment.
We are aware that many good people in perusing this chapter will think that some of the advice here given is both cruel and hard hearted; but we can safely venture the opinion that those who have reared many children, at least if they have had some nervous little ones, will be able to discern the meaning and significance of most of our suggestions. Sympathy is a beautiful and human trait and we want nothing in this chapter in any way to interfere with that characteristic sympathy of a parent for its offspring—the proverbial "as a father pitieth his children"—nevertheless, there is a great deal of sympathy that is utterly false, that is of the nature of a disastrous compromise, for the319 time being making it easy for both parent and child, but making things unutterably more difficult later on in life when both (or perhaps the child alone) must face the calamitous consequences of this failure early to inculcate the principles of self-control and self-mastery on the mind and character of the nervous child.
We so often hear "mother love" eulogized. It is a wonderful and self-denying human trait; but, as a physician, I have been led to believe that "mother loyalty" is of almost equal or even greater value. All mothers love their children more or less, but only a few mothers possess that superb loyalty which is able to rise above human sympathy and maternal love, which qualifies the mother to stand smilingly by the side of the crib and watch her little one in a fit of anger—yelling at the top of its voice—and yet never touch the child, allow the little fellow to come to himself, to wake up to the fact that all his yelling, his emotion, his anger, and his resentment are absolutely powerless to move his mother. Thus has the mother—by her loyalty to the little fellow—taught him a new lesson in self-control, and thus has she added one more strong link in the chain of character which parent and child are forging day by day, and which finally must determine both the child's temporal and eternal destiny.
System and order are desirable acquisitions for all children, but they are absolutely indispensable to the successful rearing of the nervous child, who should be taught to have a place for everything and everything in its place. When he enters the house his clothes must not be thoughtlessly thrown about. Every garment must be put in its proper place. These little folks must be taught a systematic and regular way of doing things.
Nervous children must not be allowed to procrastinate. They must not be allowed to put off until tomorrow anything which can be done today. They must be taught how to keep the working decks of life clear—caught right up to the minute. They should be taught proper methods of analysis—how to go to the bottom of things—how to render a decision, execute it, and320 then move forward quickly to the next task of life. When they come home from school with home work to do it would be best, as a rule, first to do the school work before engaging in play. In fact, all the methods which are needful for the proper discipline of the ordinary child are more than doubly needful for the training of the nervous child; while more than fourfold persistence is needed on the part of parents to make them really effective.
Whether the child be two years of age or ten years of age, when the parent discovers that the nervous system is "losing its head," that the child is embarking on a nervous runaway, or that it is about to indulge in an emotional sprawl, it is best to interfere suddenly and spectacularly. Lay a firm hand on him and bring things to a sudden stop. Speak to him calmly and deliberately, but firmly. Set him on a chair, put him in the bed, or take him to a room and isolate him.
In the case of the older children, tell them a story of the horse which becomes frightened, loses self-control, and tears off down the highway, wrecking the vehicle and throwing out its occupants. Explain to them that many of the mistakes of life are made during the times of these emotional runaways, these passing spells of lost self-control. Tell the little folks that you have perfect confidence in them if they will only take time to stop and think before they talk or act. Explain to them that since you saw that they were rapidly approaching a foolish climax you thought it was your duty to call a halt, to stop them long enough to enable them to collect their wits and indulge in some sober thinking.
Personally, we have found it to be a good plan not to be too arbitrary with the little folks, like putting them on a chair and saying, "You must sit there one hour by the clock." They usually begin to indulge in resentful thoughts and a situation is often produced akin to that of the stern father who felt compelled to go back and thrash his boy three different times during his hour on the chair, because of what he was satisfied was going through the boy's mind. No, that is not usually the321 best way. Put them on the chair with an indeterminate sentence. I prefer to carry it out something like this: "Now, son, this will never do; you are running away with yourself. Stop for a moment and think. Now I am going to ask you to sit down in that chair there and think this over quietly. I will be in the next room. Whenever you think you have got control of yourself and have thought this thing out so you can talk with me, you may get up from the chair and come into the room to me." Sometimes five minutes, sometimes fifteen minutes, and the little fellow will walk in and talk to you in a very satisfactory manner. He will give you his viewpoint and you will be able to adjust the matter in a spirit of conference which will be satisfactory to both parent and child, without doing the least violence to the responsibility of the one or the individuality of the other.
Very little is to be accomplished, when the child starts to indulge in an emotional runaway, if the parent contracts the same spirit, begins to talk fast and loud, to gesticulate wildly, grabs the child, begins to slap and shake it—that is merely an exhibition on the part of the parent of the very same weakness he is trying to correct in his offspring. I am afraid it is entirely too true that for every time you shake one demon out of a child in anger, you shake in seven worse devils. When all other methods fail and you must resort to punishment, do it with kindness, deliberation, and dignity. Never punish a child in haste and anger.
The advice offered in this chapter is not mere theory. It has been successfully used by many parents in the management of their nervous children, and while all principles of child culture must be carefully wrought out and made applicable to the particular child in question, nevertheless, the methods of repeated and firm discipline herein set forth will enable you to take many a child who has been born into this world almost neurologically bankrupt, and, by this training and discipline, enable him in adult life to draw such dividends of self-control and self-mastery as will far exceed the outward results322 obtained in the case of many children who are born with sound nervous systems, but who were early spoiled and allowed to grow up without that discipline which is so essential to later self-control and dignity of character.
In this chapter we shall consider a number of the more common diseases which are associated with the nervous system of the child. Some of these so-called nervous diseases are hereditary or congenital, while others are the result of infection and environment.
There are many conditions which cause sleeplessness or insomnia in a child aside from disturbance of the mental state or nervous system. For instance, late romping, too hearty and too late a dinner, lack of outdoor life during the day, illy ventilated sleeping rooms, too much bedding, too little bedding which causes cold extremities, too much sleep during the day, too much excitement (movies or receptions), intestinal indigestion which is associated with accumulation of gas, and constipation—any or all of these are causes of sleeplessness. Some peculiarly nervous children—those with an hereditary strain of nervousness—are easily upset or disturbed by any of the conditions above mentioned.
The treatment of insomnia consists, first, in finding the cause and removing it. Children with a nervous tendency should be let alone as nearly as possible, and just allowed to grow up as the little lambs and calves grow up. They should be fed, watered, kept clean and dry, and allowed to live their lives undisturbed and without excitement.
The medicinal remedies on the market for insomnia are all harmful if used too long or in excess, and we most earnestly urge the mother not to seek drug-store information concerning remedies for sleeplessness. The neutral bath is beneficial in324 ninety per cent of these cases. It is administered as follows: Enough water is allowed to run into the bath tub to cover the child. The temperature should be 99 to 100 F. It should be taken accurately—and should be maintained. Bath tub thermometers may be purchased at any drug store. The restless child, after the bowels have been freely moved, is placed in the water, and, without whispering, talking, or laughing, he remains there for at least twenty minutes, after which he is carefully lifted out, wrapped in a sheet and very gently dried off with soothing strokes and placed at once into his night clothes. As before said, ninety per cent of restless children will go at once to sleep after such a treatment.
Another method of treating sleeplessness is by the wet-sheet pack. Three single woolen blankets are placed on the bed and a sheet large enough to wrap the child in is wrung from warm water, about 100 F. The child is stripped and this sheet is brought in contact with every portion of his body, quickly followed by bringing the flannel blankets about him and he is allowed to remain there for twenty minutes—if he does not fall asleep before the lapse of that time. With witch-hazel or alcohol, the body is sponged off, night clothes are put on and a restful night usually follows. If fresh air is lacking, open the windows. If there is too much bedding, remove some of it. Talcum powder the sweaty back and neck and make the child perfectly comfortable. Give a small drink of water and turn out the light.
Night terrors are probably due to some digestive disturbance, with a coexisting highly nervous temperament. They oftentimes, in older children, follow the reading of thrilling stories or a visit to an exciting moving-picture show. The child goes to sleep and gets along nicely for two or three hours and then suddenly jumps up out of bed and rushes to its mother with little or no explanation for the act. In his dreams the thoughts and the imaginations of his waking moments are all confounded and alarming.
We recall one little fellow who constantly feared big, black325 birds coming in the window and attacking him—he had been reading about Sinbad the Sailor and his experiences with the big bird. He so feared this big, black bird that he could not go to sleep. For a number of nights he did not have the courage to tell his parents that it was the fear of the big bird that kept him from going to sleep, but finally he confided in his mother and told her of his fear. The mother and father both entered into a conversation with him through an open door which connected the two rooms, after the lights were out; they laughed and talked about the big bird, they openly talked of it and allowed their imagination to work with the child's imagination in planning how he could combat with the bird, should it really come, asking him how big it really was and what color he thought its eyes were and how big an object he thought its feet could carry. They all three planned a fairy story they might write which would rival the fairy stories of the Arabian Nights. In a very short time—possibly a week or ten days—the little fellow felt quite equal to these imaginary assaults, his fears were quieted and his slumbers were no more disturbed by visions of the big, black bird.
Everything should be done to relieve the stomach and intestines of laborious work during the sleeping hours, hence let the evening meal be light and eaten early enough to be out of the way, as far as digestion is concerned, by bed time.
During the formative period of the nervous system—the first few years—under no circumstances should the children be played with late at night, when they are tired and sleepy, or hungry, for it is at such times that the nervous system is so easily excited and irritated. When the baby is to be played with, if at all, it should be in the morning or after the mid-day nap. Rest and peaceful surroundings are of paramount importance to the nervous child, and he should be left alone to amuse himself several hours each day. It is a deplorable fact that the nervous child—the very one that should be left alone—is the very child that usually receives the most attention, the very one who is most petted, indulged, and pacified; all of326 which only tends to increase his lack of self-control and to multiply the future sorrows of his well-meaning but indulgent parents.
Headache attacks old and young alike, and the young infant that is unable to tell us he has a headache manifests it by rolling the head from side to side, putting his hand to his head, or by wrinkling up his brow. Headaches may be occasioned by disorders of the brain and spinal column, such as meningitis. It nearly always accompanies fever, and is often a result of constipation, intestinal indigestion, overeating, as well as eating the wrong kind of food.
The treatment of headache in children (aside from removing any known cause) consists of a hot foot bath, a brief mustard paste to the back of the neck, a light diet—sometimes nothing but water—and the administration of a laxative.
In the very young, convulsions are easily produced. That which will produce but a headache in an adult will often produce a convulsion in the child. Aside from diseases of the nervous system such as epilepsy, etc., convulsions frequently accompany gas on the bowels, intestinal indigestion, disordered dentition, an acute illness, intestinal parasites (worms), irritation about the genitals such as the need of circumcision, an adherent clitoris, adenoids and enlarged tonsils, inflammation of the ears, and poor nutrition of any sort such as rickets.
The convulsion picture is a stiffening of the body—sometimes arching backwards—rolling or staring of the eye-balls, blueness of the skin, a drooling mouth (often foamy mucus at the mouth), clinched hands, biting the teeth—if there are teeth—and even biting the tongue. There is at first a succession of quick, jerking, convulsive movements of the body which in a few moments grow less and less violent and finally cease. The child begins to cry and then soon goes off into a deep sleep, while the body seems more heavy and logy than usual. In extreme cases, the child relaxes but for a moment327 of time, when he goes off into another convulsion, sometimes going from one fit into another until death relieves him.
Treatment for convulsions must be instituted at once. Do not wait entirely to undress the child—pull off his shoes, place him at once into a good warm bath, temperature about 100 to 102 F. An ice cap should be placed to his head (cracked ice done up in a towel), and while in the bath or immediately upon taking him out, give a warm soapsuds enema. The bath that the child is placed in should be always tested with the bared elbow. A half cupful of mustard may be added to the bath. Just as soon as the child is able to swallow, give a teaspoon of syrup of ipecac. Enema after enema should be given until the water comes back clear. Undue excitement after the bath only predisposes to repeated attacks, and while the mother may be very happy that the child is himself again, under no circumstances should she caress and fondle him. Put the little one to bed and allow his nervous system to calm down; let him rest quietly and undisturbed.
Habit spasms or "tics" are common in childhood, and are caused by an over irritability of the nerves supplying certain groups of muscles. It is not at all uncommon to see a child nervously blink the eyes, twitch the nasal muscles, shrug the shoulders, constantly open and close the hand, and execute a score of other minor habit-spasms; which, day by day, wear deeper and deeper paths into his nervous system as a result of their constant repetition. These minor habit-spasms of childhood are but telltales of an unstable nervous system, of a nervous heredity lacking poise and balance; and, mind you, if this nervous system is studied, treated, and properly harnessed with self-understanding and self-control, much may be accomplished; the habit may be more or less completely eradicated. If left to itself, unchecked, the habit deepens the "spasm-groove," and the "energy-leaks" grow bigger and bigger until finally, in later, adult life, all that is necessary to convert such persons into first-class neurasthenics or hysterics is some bad news, a few worries, or a sudden shock.328
By all means study to nip all childhood twitchings in the bud; remembering all the while that childhood—the formative period for the nervous system of the child—presents the golden opportunity to prevent and abort the more grave neuroses of later life. There may be a special contraction of one or more muscles of the eyeball which produces either a "cross-eye," when the contraction is convergent, or a turning of one eye outward when the contraction is divergent. It is not possible for the mother to correct this condition. The one important thing for her to do is to take the child to a skilled ophthalmologist early in his life, that treatment may be instituted for the correction of the difficulty.
Not an unusual condition during childhood is a temporary retention of urine. It may follow an attack of colic or accompany any acute illness. Increase the water drinking, and, after seven or eight hours, hot cloths should be applied over the bladder; a large enema (enema bag should be hung low) should also be given, retaining as much as is possible. These simple measures usually relieve the condition. If retention follows circumcision, due to swelling of the parts, the surgeon should be notified.
Nocturnal enuresis (bed wetting) usually is found to "run in families." It is seldom the case to find that both the father and the mother escaped bed wetting during childhood when the child is sorely afflicted.
Early bad habits may be the prime factor in this distressing and humiliating difficulty. A little child that has been compelled to lie in wet diapers for hours at a time gradually becomes accustomed to "being wet," and the desire to urinate is not under the keen control of a will that has been trained by untiring patience to "sit on a chair" at regular intervals throughout the day. This lack of training in a child who possesses an unstable nervous system, creates the proper environment for the habit of bed wetting—which often329 marches steadily on until puberty. In the treatment of bed wetting give attention to the following:
1. The urine should be thoroughly examined.
2. The size of the bladder should be determined.
3. The last meal of the day should not be after four o'clock in the afternoon.
4. All during the day, in young children, systematic training should be begun—put the child on the chair every hour, then every hour and a half, then every two hours. Let the work be done most painstakingly and much will be accomplished toward training the bladder to "hold its contents" during the night. For a time it will be necessary to set an alarm clock to ring every three hours during the night, that the bladder may be relieved at regular intervals.
5. No liquids whatever are allowed after four p. m.; even the four o'clock meal should be very light.
6. In older children the habit is often broken by appealing to the pride—by requesting or demanding the child to rinse out the bed linen and hang it up to dry himself.
Usually at puberty the trouble ends, and while no amount of whipping will correct the difficulty, the promise of rewards, an appeal to the pride, correction of dietetic errors, the establishment of regular times to empty the bladder, the removal of all reflex causes such as adenoids, need of circumcision, worms, etc.—these combined influences—will bring results in the end, if they are faithfully and intelligently applied.
Cerebro-spinal meningitis is not highly contagious. Children old enough to complain of symptoms usually first complain of an intense headache with frequent vomiting and very high fever. Great prostration is seen, the pulse is weak, the respirations are irregular, the child may have convulsions, or it may have chills and fever, and rigidity of the body may be present. The position of the child is very characteristic. It does not want to lie on its back but usually rests on one side, with the spine more or less arched. It is a very serious disease and demands the early attention of a physician. Some cases are330 very mild and others are exceedingly grave. If the physician is secured early, and special remedies administered that are known today, many of the children may be saved.
Infantile paralysis is a serious disease of the spinal cord which comes on very suddenly and is associated with vomiting, pain in the legs, and a high temperature. After these symptoms have lasted a day or two the paralysis is discovered. There may be convulsions. The paralysis is progressive, and the wasting of the muscles increases until by the end of a couple of months one limb is considerably shorter than the other. Sometimes the baby goes to bed at night in apparent good health and wakes up in the morning paralyzed.
In this disease the attention of the best physician in your community should be called to the case at once, for there are being developed in our large research laboratories special vaccines for this condition as well as for spinal meningitis. But what is done must be done very, very early, so let there be no delay in calling in medical counsel.
There are other forms of spinal paralysis which, associated with tuberculosis of the spine and other spinal diseases, result in loss of power to one or more groups of muscles. The only treatment that can be given in the home is to keep all of the paralytic portions of the body very warm by external heat, care being taken to avoid burning, and secure medical advice. Often, later in the course of the disease, by the aid of crutches and braces, the child can be taught to go to school and to get around the house about his little duties.
The slight facial paralysis which is so often seen in babies that have been delivered with forceps, usually clears up in a few days or at the latest in a few weeks or months.
Saint Virus' dance (chorea) is a peculiar disorder seen in nervous children, and which usually clears up in a few weeks or months under proper treatment. It is characterized by irregular jerkings pretty much all over the body, so that the331 child staggers as he walks, drops his food at the table, and executes many other noticeably abnormal movements. The child should be taken out of school at once and removed from association with children who might make sport of him or otherwise annoy him and thus increase these irregular jerkings. He should at once be put under the direction of competent medical authority. Simple food, colon hygiene, more or less complete rest, and freedom from annoying circumstances, will usually bring about a speedy recovery.
Water on the Brain is characterized by an enlarged head due to an increased accumulation of fluid within the cranium. While the face remains small the head greatly increases in size so that oftentimes it must be braced while the child is compelled to remain in a wheel chair. The mentality is usually fairly normal, but the enormous weight of the head compels the life-long occupancy of a wheel chair.
Deaf-Mutism. The child born deaf pays no attention whatever to sounds. An intellectual expression is seen on his face and by six months he is able to do all that a normal baby can do with the exception of hearing. The child should early be taken to an ear specialist in the endeavor, if possible, to correct the defect of hearing. Such little ones who are destined to a life without sound, should be given every opportunity to learn to read the lips and to secure a good education—to be taught a vocation where eyesight is of more value than hearing. Special institutions are in existence today which can take these deaf mutes when small and so teach them to make audible sounds that they can make themselves understood—at least partially. Lip reading is a wonderful improvement over the deaf and dumb alphabet, and should be taught early.
Congenital Blindness. Perhaps not until the child is six months old can the observer distinguish between blindness and idiocy. The blind child of course will not fix his eyes upon any object; but the general lassitude and the inability to hold up its head, while seen in idiocy, is not present in blindness.
Feeble Mindedness. A baby that is born with a weak mind332 is found to be very backward in all the normal developmental attainments of the growing child. A normal baby holds up its head at four months and should be able to sit erect at six months. The weak-minded baby will not do this, and often as late as two years it will not make any attempt to walk or to talk. There is an unnatural expression—a vacant look—to the face, while there is often much dribbling at the mouth.
Early Training should be Instituted. It is necessary to call the attention of a physician to these facts, that the parents may be instructed in regard to the early training which is so essential in all these weak-minded little folk. In our opinion it is best to remove these children early to special institutions, where their education can be superintended by those thoroughly accomplished and accustomed to dealing with this class. There are varying grades of feeble mindedness—the backward child who requires a longer time to learn things, and the child who is slow at school and possibly cannot get through more than the fourth or fifth grade—but as soon as weak mindedness is discovered, it is best to transfer the child to some special institution.
One of the earliest skin troubles that the average normal child suffers from is prickly heat—a tiny, red-pointed rash always accompanied by sweating and usually resulting from over-dressing, stuffy rooms, and other conditions that make the child too warm. Prickly heat produces more or less discomfort but usually little or no itching. Ordinarily, a sponge bath followed by the application of talcum powder is sufficient to give relief in mild cases; but severe or neglected cases should be treated by means of bran baths, a cupful of bran being tied up in a gauze bag and suspended in water until the water assumes a milky color. Soda baths, two tablespoons to a gallon of water, are also very soothing. A baby should never receive any friction with a towel after such baths, but should be rolled up in a clean linen towel and simply patted dry.
Great care should be exercised in the choice of baby's soaps. Among a number of soaps that might be mentioned castile soap is, perhaps, as good as any. Frequent sponging is required to wash off the irritating perspiration; cool clothing, plenty of talcum powder, a dose of calcined magnesia, and a regulated diet are necessary to clear up the trouble.
Chafed skin, particularly between the buttocks or in other folds and creases, should be kept free from soap. Either the starch or bran bath may be tried, while olive oil should be frequently and lightly rubbed over the chafed part. A bit of sterile cotton placed between the folds to prevent friction is often all that is necessary to correct the difficulty.
Dandruff or milk crust which is often seen on young babies'334 scalps has been described in detail elsewhere. It should early receive the vaseline rub at night which will often loosen up the hardened crusts. It may be gently removed in the morning with soap and water unless the case has gone on to great severity. In such neglected cases the mother should not undertake to correct the difficulty alone. Taken early, when the scalp is covered with tiny flakes known as milk crust, it can be quickly relieved.
Vulvovaginitis is a very contagious disease, and before the days of hospital asepsis, which is so perfectly maintained today in our large institutions, this disease used to go right through a children's ward because of carelessness in the handling of soiled diapers, etc. The sign of this disease is a yellow-white vaginal discharge, while the surrounding skin covering the inside of the thighs and buttocks may be very much reddened. The baby should be taken at once to the physician at the first appearance of these symptoms. Only rigid isolation can possibly prevent other children from getting it—essentials are separate towels, wash towels, soap (in the case of the older children), and, in the case of the baby, separate diapers and rigid scrubbing of the attendant's hands—in this way only can this infection be held in check. The infected child should sleep by herself, and utmost care must be exercised in preventing her fingers from first touching the itching vulva and then placing them to the eyes or to the mother's eyes. A vulva pad must be worn as long as the disease lasts. The physician will give you the proper medicines to be used in these cases, and if no physician is within reach, you are perfectly safe in dropping into the spread apart vulva a few drops of twenty-per-cent argyrol and then applying the vulva pad. After each treatment the hands of the mother or nurse must be most rigidly cleansed.
Eczema is a very troublesome disease, particularly in infants; there are so many forms of it that there is neither time nor space in this volume to describe them individually. This dis335ease may be produced in children by either internal or external causes—from friction on the skin, from coarse, rough woolen clothes, or from starched garments, or from lace or starched bonnet strings which rub into the folds of the skin. Irritating soap, the contact of soiled diapers, cheap toilet powders, and discharges from the nose and ears may also be responsible for the disease. The particular internal causes are over-feeding, digestive disturbances, the too early use of starches which create fermentation in the intestinal tract. In the most frequent form of eczema the skin becomes red and then there appear tiny vesicles (water blisters) which soon rupture and "weep." This fluid which oozes from these tiny, ruptured vesicles, in connection with the perspiration and exfoliation of old skin, forms heavy crusts upon the face which are both unsightly and annoying.
Another form of eczema is simply a very badly chafed condition accompanied by intense itching, and commonly known as "dry eczema." A very disagreeable form is the pustular variety. One poor little sufferer that was once brought to us had so many pustules on his head that one could not put a ten cent piece on his scalp without touching a pustule. The treatment of these cases, in order to be effective and leave the child's head in normal condition, must be administered with the utmost patience every day for weeks. A doctor's help is always required in combating this sort of skin trouble. If the cause is external, then the clothes should be changed. All irritation should be removed—the clothing must not be allowed to scratch the skin. The child must not scratch himself. If necessary, little splints may be placed on the inside of his arms to prevent his bending the elbows if the eczema is on the face, while the little sleeves may be pinned to the side of the dress to resist the movement of the arms.
The diet should be most carefully looked into. The nursing mother will earnestly look into every article of food she herself is eating, and carefully avoid all foods that produce fermentation or decomposition. The mother's urine should be336 examined and its acidity noted; if it is above normal she should take some alkalines such as ordinary baking soda or calcined magnesia. If it is a bottle-fed baby, any form of flour should be removed from the food and the quantity of the milk reduced. All this, of course, is done under the direction of the physician. Repeated doses of castor oil may be given.
The name of the medicinal agents that have been used in the treatment of eczema, is legion. Perhaps one of the most widely used is the early varnishing of the affected skin with ichthyol (one part ichthyol, one part distilled water), which is swabbed on after the skin has been cleansed with olive oil. Allow this to almost dry, and then sprinkle on talcum powder which smooths over the dry varnish of ichthyol. This is worn every night and during the day, in bad cases, even when the eczema is on the face. It is renewed each day, and is preceded by the olive-oil bath. No water or soap is ever used in eczema. Fortunately, the Eskimo has taught us that the skin really can be cleansed with oil as well as with water. In the appendix will be found two prescriptions, number one and number two, that have proved very beneficial in some of the most severe forms of eczema.
Hives, a crop of little raised red papules closely resembling lesions caused by the sting of a mosquito, may make their appearance upon the skin of the child, remain a few hours, and then disappear. Hives are usually due to digestive disturbances and may be caused by such foods as strawberries, nuts, pastries, pineapple, certain sea foods, mushrooms, etc. A good cathartic, the taking of alkalines, such as baking soda or calcined magnesia, with a bran or starch bath, or possibly a soda bath, will usually correct the difficulty. The same treatment may be used in nettle rash or prickly heat.
Freckles seem to run in families. Broad-brimmed hats or sunbonnets may be worn, but under no circumstance should a little girl be bidden to remain in the house and shun the beautiful, sunshiny outdoors just because she freckles easily. Do not apply any lotions to the freckled face without medical337 advice, for great harm may be done the tender skin of the child.
Often upon the scalps of young children may be seen circles—rather, patches—which are slightly rough to the touch, and which cause the hair to fall out and the spots to remain bald. They are known as ringworms of the scalp. The affection may likewise appear on the body or the face, presenting a ring of reddened skin with a scaly border. Ringworm on the scalp is hard to treat and medical help should be secured, for, in spite of all that can be done, the disease often runs its course, leaving round bald spots over the head. Ringworm of the face, taken early, is helped by carefully painting with tincture of iodine. The mother should constantly bear in mind that ringworm is a "catching" disease, so that all handkerchiefs, towels, and clothes are to be kept separate. The disease known as mange which so often attacks dogs, is nothing more than ringworm, and children often contract the disease from dogs. Ringworm, whether it be on children or dogs, may be greatly helped by the use of tincture of iodine and other appropriate remedies.
The much poulticing of boils has done an untold amount of mischief. Many children and adults are in their graves today because of improper treatment of boils. Blood poisoning which so often follows the careless poulticing, as well as the uncleanly opening of boils, can all be avoided. Before touching a boil, the surrounding skin should be thoroughly washed with sterile cotton and laundry soap and then disinfected with alcohol. Then, with a scalpel or a surgeon's knife which has been either boiled for twenty minutes or allowed to remain in pure carbolic acid two minutes and then in alcohol two minutes, it should be thoroughly opened down to the core so that the pus may come out. It is very much better for the trained hands of a physician to do this than for any member of the family to undertake such an operation—where the danger of blood poisoning is always present. The only treatment of skin eruptions338 containing pus which is justifiable for the home folks to undertake is to simply paint them with iodine. Under no circumstance should poultices be used.
It is not at all uncommon for small children to develop a group of fever blisters on the lips when suffering with any disease, or experiencing a high fever. Even a simple cold or a spell of indigestion may be accompanied by fever blisters. They appear not only on the lips but also on the edges of the nose and may even be seen on the chin.
Early in their first appearance they may be treated with spirits of camphor or plain alcohol, which sometimes tends to abort them; but they usually run their course, and when they are fully developed they may be treated with zinc oxide, simple borated vaseline, or ichthyol.
Very often children's hands are disfigured by warts. They appear suddenly, develop rapidly, and many times disappear just about as suddenly as they appeared. Every child suffering from warts usually passes through the stage of charms and lingoes which are popularly used to remove these disagreeable growths. We hardly see any efficacy in "bean-ie, bean-ie take this wart away," or any particular virtue in stealing mother's dishcloth, cutting it up into as many pieces as there are warts on the hand and rubbing each wart with a separate piece of the cloth; but you will find people in every town or village who will assure you that their warts were driven away by one of these charms or lingoes. Warts are either better left alone or removed by a physician with the high-frequency spark or some other reliable method.
A red or purplish patch on the skin is the result, as mentioned in an earlier chapter, of an embryological accident in which one or more embryonic cells slipped out of place in the early days of skin formation. These accidental markings may339 occur on the face, the scalp, or on any other portion of the body, and they should be let alone, unless they show a tendency to grow, when it may prove best to give them proper surgical attention.
A mole is also a birthmark, and if found upon the neck or shoulders where it is likely to disfigure, it may be removed by the high-frequency spark, or by surgery, in the same way as warts. Never tamper with moles. Leave them alone or turn them over to the surgeon.
Erysipelas is a much-dreaded disease which is the result of infection with the blood-poisoning germ—streptococcus. It usually occurs about a wound, and is due to infection by this microbe. If it follows circumcision, it is due, of course, to infection, and may be very serious, even causing death. It attacks persons of any age and is oftenest seen on the face. In appearance, the skin is a bright and shiny red, with a definite line of demarcation slightly raised at the edges because of the swollen tissues underneath. On pressure, the redness disappears but reappears immediately upon relieving the pressure. The inflammation, pain, and fever often continues a number of days, during which the child should be isolated from all other members of the family. The bowels should be freely opened, and the diet should be liquid and soft; while local treatment is cared for by the physician who should always be called. Should erysipelas develop on a very young baby it is very important that he should be removed at once from the mother. As stated before, the disease is produced by the blood-poisoning germ which is very much to be avoided in any and all stages of obstetrics. One attack in no way renders the patients immune. They may have repeated attacks of erysipelas. The treatments should be started early and kept up most rigidly.
In thickly settled districts among the poor and uneducated, where filth and untidiness reign, the "itch" is a very prominent disease. It is caused by the itch mite, a parasite which340 burrows underneath the skin leaving behind its eggs in little irregularly shaped, bluish tinted ridges. Such a profound itching is set up by this burrowing and depositing of eggs that the child cannot resist scratching, and all taken together produces the typical itch-rash. The common site for this rash is on the sides and between the fingers and toes; on arm pits and buttocks of the child, as well as at the waistline. The treatment is usually beyond home remedies. A physician should have charge of the case who will conduct a line of treatment which, if diligently followed, will rid the body of this scourge within a week or ten days.
Along with the itch are often found parasites of the head, or lice (pediculi). It is not at all infrequent to find them in the heads of uncared for children; but if a much-cared-for child is brought in contact with an infected head he will probably "catch" the infection. A most intense and disagreeable itching is set up at once. The treatment consists in getting the head clean by the use of a very fine comb, thus endeavoring to remove the adult parasites as well as the eggs or "nits." However, great care should be taken to avoid injuring the scalp. Perhaps the simplest and most effective treatment known is the kerosene bath which should be applied at night, the hair being done up in a bandage until morning, when the kerosene is washed off with soap and water and then the hair given a vigorous vinegar shampoo in order to destroy the "nits." Tincture of larkspur, or an ointment made from the seeds, may also be used. It is applied several days in succession and then washed out.
Reference has already been made to certain accidents of embryology during the very early days or weeks of the formative period of the embryo. Common illustrations of such deforming developmental accidents are harelip, cleft palate, and club foot.
In the case of a partial or complete failure of the two sides of the face to come together in the median line, a deformity results which is known as harelip—a partial or complete cleft of the upper lip. It may be a single or a double cleft, exposing the teeth, or the cleft may even extend up into the nose. This deformity may seriously interfere with nursing, making it necessary to resort to feeding with a medicine dropper and later a spoon. The success of the operation for the relief of harelip, which should usually be performed during the early months of life, is often very remarkable.
Should this failure to unite be in the deeper structures of the head, then cleft palate is the result. This, too, may be partial or complete: partial as seen in a cleft of the soft palate only; and complete, when the hard palate also is involved. In such an instance it is the floor of the nose that is defective; hence the nose and mouth are one cavity.
A specially devised apparatus which assists the child in nursing may be found on the market, for nursing is well-nigh impossible without the closure of the roof of the mouth. The operation for cleft palate is usually successful when performed at the proper time and by competent hands.
In tongue-tie the weblike membrane underneath is attached342 too far forward, so that the child is quite unable to protrude his tongue, and this condition greatly interferes with sucking. The operation for the relief of this condition is slight, and should be performed as soon as the defect is discovered.
Occasionally there is a webbing of one or more fingers of the hand, and there are sometimes seen too many fingers or a double thumb. It is needless to allow such a deformity to continue; the operation for relief is often remarkably successful and should be performed very early.
Clubfoot results when short tendons or contracted tendons pull the toes inward or outward with raising of the heel. Treatment must be instituted early; braces or splints are applied; and untiring efforts are put forth in massage and other lines to prevent a lifelong handicap of clubfoot.
An inward rotating of the legs presents the deformity of pigeon-toe. The normal foot naturally inclines toward "pointing in," and such a condition should not be discouraged. Many flat feet (broken arch) are due to shoe lasts which compel the toes to slant "out," and the bunions which so often follow such mistreatment may be exceedingly painful.
By all means place shoes on the pigeon-toed child that possess straight lasts with flexible arches, and which admit of the exercise of many muscles of the foot which otherwise remain inactive.
As the child grows older the toenails thicken, and often in their trimming they are cut so closely at the corners that sometimes a condition results known as ingrowing nails. Such are very painful and must receive special attention. First of all, the nail is cut squarely, and after scraping it thin the corner is lifted and cotton so placed under it that the nail's downward and inward growth is stopped.
Curvature of the spine is more common than is usually thought. The most frequent variety of it is the lateral curvature. One shoulder is lower than the other, and the hips343 are therefore uneven. Rickets, during infancy, is the most common cause of spinal curvature.
Improper sitting at school—sitting on the edge of the seat—or carrying heavy loads are often contributing factors to the production of lateral curvatures. Only the muscles and ligaments enter into this deformity, hence the treatment should be started early and should consist of:
Pott's disease, or tuberculosis of the bone, often results in an angular spinal deformity. This curvature, unlike the lateral curvature, is a sequela of an actual disease of the bones. It is always very serious and demands early treatment from skilled hands. Early in the disease there is a peculiar stiff, tottering gait. The little child holds the spine rigidly, and in picking up objects from the floor bends the knees instead of the spine. If the trouble is in the upper spine, the shoulders are held high and the head is stiffly poised, it is never rotated; in looking about the entire body turns.
Medical aid should be secured early. The X ray not only locates the difficulty but also determines the extent of the process. If the spine be put to perfect rest, outdoor life begun, a diet rich in fats established, the results are often wonderfully successful.
Another tubercular condition is seen in the much dreaded hip-joint disease which parents should always be on the lookout for. The earliest symptoms are crying out in the night suddenly, unnatural standing on one leg (to relieve the strain on the diseased hip) and so-called "growing pains." Call in a physician very early and institute proper treatment. A pos344terior curvature of the spine is often associated with a bad case of rickets. It is of temporary duration, and usually clears up when the symptoms of rickets have been eradicated. It involves only the back muscles—not the vertebral bones.
The young mother is often very much concerned over the misshapen head of the child as a result of a prolonged labor; and it does seem quite miraculous to see a head, more nearly resembling an egg than anything else, become beautifully round and shapely by the end of two or three days.
Protruding ears may be encouraged to lie more flatly by the wearing of a specialized bonnet at night. When the babies are too young to turn themselves they should be turned first to one side and then the other, while care should always be exercised in properly straightening out a curled under ear or an overlapping ear.
While we so often regard rheumatism an adult disease, nevertheless, children do suffer its aches and pains as well as the fever which so often attends the inflammatory type. The so-called "growing pains" are often of rheumatic origin.
Diseased tonsils not only are often—very often—the avenue of entry of infectious microorganisms that cause one type of rheumatism, but many forms of valvular heart disease are also directly traceable to these same diseased tonsils. The treatment consists in giving proper attention to the tonsils, even removal if necessary—and if the child is old enough. All other possible causes should be located and removed; the child should have absolute rest in bed with brisk cathartics and a liquid diet (no meat broths). The diet should consist more of alkalinizing foods as shown in the special table in the appendix. Medicinal alkalines are often given when the urine shows a very high acid reaction.
Scurvy, seen in children who subsist on "prepared foods," is manifested by tender legs and swollen gums which have a tendency to bleed easily. Pallor, loss of appetite, and insomnia345 accompany the condition. The treatment of scurvy is change of diet from "patent foods" to fresh cow's milk, with the addition of orange juice, daily. In older children the food must be very nutritious; out of door life, salt glows, friction baths (see appendix), and the taking of large amounts of fats are all essential to the cure.
Enlarged glands, or what our grandmothers used to call "kernels" in the throat are often the result of inflammation in the mouth or throat, and occur in connection with many of the childhood diseases, notably diphtheria, scarlet fever, and scarlatina.
Glands appearing in the back of the neck may be occasioned by pediculli (lice), ring worm, or eczema, while those seen in the neck just back and below the ears may come from mastoiditis (inflammation of the middle ear) or adenoids.
Glands felt under the arm enlarge because of trouble or infection in the breast, hand, or arm; while glands in the groin are usually due to some infection of the feet, legs, or abdomen.
These glands usually disappear when the general health and well-being of the child is improved by:
Rickets (a disease of the bones) often follows in the wake of faulty feeding and unhygienic surroundings. The bones lack a proper amount of lime salts and other elements. Development in general, especially that of the bones, is greatly interfered with.
Bowlegs, prominent square brow, enlarged perspiring head, weakness, and often tenderness of the flesh, are notable signs of the disease. The treatment varies little from that346 of scurvy, and will be provided in detail by the attending physician.
Children often suffer from malarial parasites. Sudden rise of fever on regular days (sometimes daily, every two days or every three days) should demand a careful medical examination including the examination of the blood where the offending organism is seen in the red blood cells. We recently saw a little girl who happened to have an earache and was about to be operated on for ear trouble, when examination of the blood revealed the fact that she was suffering from malaria.
In the routine examination of adult patients, the X ray observations of the lungs often reveal deposits of lime salts which tell the story of a successful fight against tuberculosis (Fig. 16). And while it may seem surprising, we believe beyond a doubt that most of us have had some varying degree of tuberculosis while young—the unrecognized battle has been fought—and these small monuments of lime salts alone remain to tell the interesting story.
The pity of it is that whole armies of little folks fall in this struggle against disease, for it is one of the common and fatal diseases of childhood. Fresh-air schools, playgrounds, and free school lunches are saving hundreds of children from the ravages of this disease each year.
Tuberculosis is strictly a house disease, hence the little tubercular patient must seek outdoor life. All avoidable exposure to the disease must be denounced, and public sentiment must continue to be aroused to the hygienic betterment of the tenement districts and basement homes. The sanitary drinking cup and the bubble fountain must be encouraged, as must also the proper ventilation of all places where crowds assemble, be it the schoolroom, the theater, or the church.
While tuberculosis is known as the "great white plague," syphilis and gonorrhea constitute the "great black plague," 347which seen in the little folks is pitiable indeed, leading us to realize that surely "the children's teeth have been set on edge" because of the careless eating of sour grapes by the parents. Syphilitic parents who have not been properly treated, should think many times before they take upon themselves the awful responsibility of bringing into the world a tainted child. Proper mercurial treatment should be instituted at once not only for the child but also in the case of both parents.
In this chapter we wish to instruct the mother or the caretaker in doing the one thing needful for every one of the more common household accidents and emergencies while waiting for the doctor.
In every household there should be found an accident and emergency "kit" of necessary paraphernalia for the quick application of the one necessary medicine, dressing, etc. This "kit" should contain baking soda for burns, bandages and sterile gauze for cuts or tears, together with adhesive plaster, needle and thread, etc.
Far greater harm is often done the skin by the subsequent scratching of the insect bite with dirty finger nails than by the bite itself; and so it is very important that we remember to allay quickly the intense itching by the application of ammonia, water or camphor. Almost instantly the itching is stopped, and the added "scratching" irritation to the already injured skin is thus avoided.
By the aid of a magnifying glass, and often by the naked eye, we may detect the stinger which has been left behind by the greedy guest, and which should be removed by a pair of tweezers. Ice-water compresses will stop the swelling and even an old-fashioned mud dressing, which was used and appreciated by our great grandmothers, is a thing not to be despised.
If the much admired shrubbery be removed one hundred feet away from the porch, mosquitoes would trouble the household less. It has been demonstrated in many localities that clearing away the near-by clumps of shrubbery permits the family to349 sit on unscreened porches unharmed. Mosquitoes multiply rapidly in stagnant pools of water, but if oil is poured over these stagnant waters the increase of mosquitoes is abated, and their total extinction is not unheard of in swampy districts receiving such care.
Whenever baby is out of doors where mosquitoes, flies, or other insects are to be found, he should be properly protected from such pests by mosquito netting stretched over a frame eighteen inches above his face, for we can think of nothing more uncomfortable than a mosquito netting dragging over a sweaty baby's face. The fact that mosquitoes, flies, roaches, and other insects are carriers of tuberculosis, infantile paralysis, typhoid fever, cholera, yellow fever and malaria, as well as a host of minor ailments, should make us the more anxious for either their extermination or the protection of our children from their greedy bites and stings.
Dogs, cats, rats, or mice bite at any time of the year, and provision should always be made for ample protection against such accidents.
Such a wound should always be squeezed or sucked until it has bled freely, and then be cauterized by a red-hot iron or touched with an applicator that has been dipped in sulphuric acid or nitric acid. A subsequent dressing of Balsam Peru is healing. The dog should be watched, and if it shows signs of hydrophobia the bitten child should be promptly taken to the nearest Pasteur Institute for treatment.
In the case of snake bites the same sucking and cauterizing treatment is indicated, with the additional tying of a handkerchief or cord a few inches above the wound to stay the progress of the blood and to keep the poison out of the general circulation. A solution of twenty-per-cent permanganate of potash should be used to wash the wound.
The popular administration of large draughts of whiskey is of no benefit, for the secondary depressant effect of alcohol increases the body's poison burden, and those who survive do so in spite of the whiskey, and not because of it.350
Small articles such as buttons, safety pins, thimbles, coins, etc., are often swallowed by little folks, and if they lodge in the throat and the child struggles for his breath the treatment is as follows: grasp him by the heels and turn him upside down while a helper briskly slaps him on the back. The foreign body generally flies across the room. If it is lodged high up in the throat it may often be dislodged by the thumb and finger. If it cannot be reached and it will not go down, lose no time in seeking an X-ray laboratory where its exact location may quickly be discovered and proper measures instituted for its removal.
A troublesome fish bone is easily dislodged by swallowing a half-chewed piece of bread which carries it down to the stomach. Cathartics and purgatives are not to be given; in due time the object will appear in the stool. In all instances it is well to locate its exact position by the X ray—that there may be assurance that it will do no harm.
It is surprising what large objects can be swallowed. One old gentleman swallowed his false teeth, and a six months old baby swallowed, or at least had lodged in its throat, a silver dollar.
All detachable parts should be removed from toys that are given to babies, such as the whistle from rubber animals, the button eyes of wool kittens and dogs, and other such removable parts.
To begin with, do not get "panicky," but carefully, painstakingly, and patiently do the following:
1. Rub the well eye until the tears flow plentifully in both eyes.
2. Blow the nose on the injured eye side, closing the other side. This often encourages the tears to wash the foreign speck down through the tear duct, into the nose and out into the handkerchief (in case the child is old enough to follow such instruction). If the foreign body be sharp, as a piece of steel or flint is likely to be, it may be driven right into the eyeball.351 Seek a physician who will drop medicine into the eye to deaden the pain and then if it cannot be gently rubbed off the eyeball, a magnet will promptly remove it.
An eye bath of warm boracic acid is always comforting and never does harm, so that may be given while waiting for the doctor to come, if the object seems to be beyond the reach of family help.
If an alkaline, such as lime, be blown into the eye it is very painful, but much relief may be obtained by gently pouring into the eye, by means of a medicine dropper or eye cup, warm water to which has been added a little vinegar or lemon juice. Likewise, acid in the eye produces much pain. In this instance, an eye bath of a weak soda solution is indicated.
Insects that have crawled into the ear may be suffocated by dropping sweet oil or castor oil into the ear, which, after twenty minutes, should be washed out by gentle syringing with warm water from a fountain syringe, hung one foot above the child's head.
Peas, beans, shoe buttons, or beads are sometimes put into the ear and nose by adventurous or experimenting children.
The shoe button or bead will not swell as does the pea or the bean, and may often be safely washed out. If it is causing no pain and will not drop out in case of the ear, or will not be easily blown out in case of the nose, see your physician at once. He has in his possession just the necessary instruments for its immediate removal.
Peas and beans swell, and consequently cause greater discomfort the longer they are in; do not poke at any foreign body lodged either in the nose or the ear, for the ear drum may thus be injured, while in the former case it may be pushed into one of the accessory sinuses.
One of the most comforting and highly effectual forms of heat for an aching ear is a four-candle-power carbon electric light on an extension cord that permits the light to come in close352 contact with the ear. A shade is made from a piece of stiff letter paper that fits the socket snugly and flares out to a three inch opening, which should extend below the point of the bulb one inch. This shade holds all the heat and light and directs it into the aching ear.
In every well-ordered household there will be found a three-per-cent solution of carbolic acid and glycerine of which one drop should be put into the aching ear, and then the external heat, mentioned above, should be applied. A bag of warm salt, a hot water bag, or a warm plate will provide external heat if an electric light is not available. Do not put laudanum or other remedies into the ear, other than are herein suggested, without your physician's knowledge.
Earache is always serious, and since it is usually indicative of trouble which, if left untreated, may cause deafness, it demands thorough treatment from skilled hands.
Running ears invariably need medical attention and should never be neglected.
If the nose bleeds whenever it is cleansed, more than likely there is an ulcer on the septum which will continue to bleed if left untreated. The physician should heal the ulcer, and the child should be taught always to vaseline the nostril before cleansing it.
In case of persistent nosebleed, put the child to bed with the head elevated. Pressure should be put on the blood vessels going to the nose by placing two fingers firmly on the outer angles of the nose on the upper lip, while a helper may put firm pressure at the root of the nose at the inner angle of each eye. An ice bag may be placed at the back of the neck, and another piece of ice held on the forehead at the root of the nose. If these measures do not stop the flow of blood a few drops of adrenalin may be put into the nose and repeated in five minutes if necessary. As the bleeding begins to stop, as well as during the bleeding, all blowing of the nose is forbidden as it will only cause the bleeding to start afresh. It sometimes helps to hold a piece of ice in the hands.353
A cut with smooth edges, if deep, should be allowed to bleed freely, should be washed in boracic acid solution, and its edges held together by a stitch which is usually put in by a physician; but if treatment is to be given at home, the hands of the nurse must be thoroughly washed and the thread and needle boiled for twenty minutes. If the physician has been sent for, make firm pressure over the wound by bandaging tightly with a dressing of sterile gauze dipped in boracic acid solution.
In case of a slight cut, make it bleed freely, then wash in boracic-acid solution and apply sterile gauze held in place by a binder. If no odor or pain follows, let alone for two or three days, when a new dressing is applied.
A physician should be called in case of ragged wounds or tears, as such usually leave bad scars. Cleanse carefully, leaving no dirt in the wound, cause it to bleed, if possible, and apply a sterile gauze compress wet in boracic-acid solution, bandaged on as directed above. Zinc ointment may be applied to surfaces that have been skinned. All dressings on dirty wounds should be changed daily.
Blood poisoning may readily follow a wound, hence the utmost cleanliness should prevail. The hands of the attendant, the dressings, the surrounding skin, must all be clean. The bowels should be kept open, and under-feeding rather than over-feeding is indicated.
If a needle be needed to open a sore or boil, always disinfect the part and surrounding area by painting with tincture of iodine, and heat the needle to red heat through a flame before it touches the sore.
In case of cuts or wounds of the eyeball apply a compress of sterile gauze wet in boracic acid, held on by a bandage, and go immediately to a good eye specialist.
Wounds made by pins, needles, fishhooks, tacks, and splinters are always very painful and great care must be exercised to force bleeding freely, which helps to wash out infection, as354 more than likely microbes entered with the instrument or sliver when the wound was made.
Fishhooks are exceedingly troublesome, as they often occasion the enlarging of the wound to get them out, especially if they have gone in beyond the barb.
Slivers are easily broken off, so great care is needed in their removal. A pair of tweezers is convenient for seizing the protruding portion, while all side movements are avoided lest it break off in the flesh, in which case it may be gotten out with a needle that has been sterilized in a flame.
All puncture wounds should be dressed with the wet, sterile compress, covered over with wax paper and bandaged loosely; this encourages cleanliness and favors healing.
If left untreated, bruises swell, become highly discolored, and in the process of healing pass through the dark blue, green, and yellow stages. The treatment is as follows: Apply hot and cold alternately—the heat should be as hot as can be borne and left on very hot for three minutes, then ice water compresses should be applied for one minute, then hot again—these changes should continue for an hour, and if carried out immediately after the injury all discolorations and most of the swelling may be avoided. Witch-hazel compresses are comforting. If discoloration has taken place, the application of hot compresses will often hasten its disappearance.
While there is very little a member of the family or a non-medical friend can do in case of a fracture, and while it is unwise to offer suggestions relative to the setting of bones, yet it is highly important that both the family and friends know how properly to support a broken leg while carrying a disabled person into the house or to near-by medical aid.
For instance, in the case of a fractured leg below the knee, if a couple of flat boards three inches wide be tied about the leg with two pocket handkerchiefs, the ends of the fractured bone will not rub against each other and the pain will be355 much less in carrying. In this way all danger of causing the broken bones to protrude and thus "compounding" the fracture is also avoided. And also, if there is no near-by ambulance, a good emergency stretcher may be improvised out of two or three buttoned vests with two poles, rakes, or brooms run through the armholes—one vest under the shoulders and one under the hips and still another under the fracture. An injured person may in this way be carried for miles quite comfortably.
Two people may fashion a seat out of their four hands on which the disabled child may sit with his arms about the necks of his two friends. If the fractured end of the bone penetrates the flesh it is then known as a compound fracture and the utmost cleanliness must prevail—as in dressing other wounds. An X ray laboratory should always be sought, where convenient, to ascertain if the ends of the bones are in good position.
In dislocations, the bone has slipped out of place at the joint. Medical aid should be called to replace the bone, while hot applications may be used in the meantime.
All sprains (a twist or straining of a joint) should promptly be put into a very hot bath and held there for thirty minutes. If this is impossible, then a rubber tube or a handkerchief is tied snugly between the sprain and the trunk of the body. Almost instantly the pain, which is often intense and severe, is very much lessened. The hot-water bath is very hot, and the joint should be very red on taking it out. Immediately following the bath the injured joint is wrapped in a very cold wet compress, which is next completely covered by silk, gutta-percha, mackintosh, or many thicknesses of newspaper—anything that will hold all the heat in—as the cold compress is quickly heated up. Lastly, a bandage of heavy flannel completely covers the whole—compress, impervious covering, etc.
The joint is now elevated for three hours, when it is again immersed in a very hot bath and then again the cold compress is applied. This is continued every three hours, except during sleep, for two days, after which it may be done morning and356 evening. Massage is now administered every three hours, first four inches below the injury then four inches above it, while in a day or so the joint itself may be gently rubbed with well-oiled hands. By the end of one week the patient begins to use the injured member.
In the case of a sprained ankle a properly applied adhesive strap bandage will give no end of relief and support. Various liniments may be applied, but usually the good obtained is from the thorough rubbing which always accompanies their use according to directions.
Sprains treated as above directed will often liberate the child in one-third the usual time generally allotted for its healing.
Keep the child who has frozen some part of his body in a cool room, and rub the frost-bitten part with snow or ice water, or wrap it up in cold water compresses.
The return to heat must be slow indeed, else much pain may be experienced; blisters followed by discoloration, and even mortification, may set in. You may be surprised some morning on awakening to find your child's hand twice its normal size and very red, because it was out from under the cover a good share of the night exposed to Jack Frost. Do not bring it to heat quickly but immerse it in cold water, gradually and slowly raising the temperature of the bath until it is warm and comfortable.
The intense itching and burning of a chilblain may often be relieved by painting with iodine or triple chloride of iron (Monsel's solution). Soap liniment has also been suggested, as well as alternate applications of hot and cold water. Chilblains are troublesome, painful, and their yearly recurrence is often very annoying.
Poisons of an acid nature, such as hydrochloric, sulphuric, nitric, or oxalic acids, are neutralized by alkalines, such as magnesia, chalk, soda, and soap, followed by soothing drinks or sweet oil.357
Remember that carbolic acid is not an acid, and is not antidoted with alkalines. The swallowing of carbolic acid should be quickly followed by diluted alcohol, and if this drug is not ready at hand many of the numerous alcoholic patent medicines will do just as well. Epsom salts should be given in abundance.
Poisons of an alkaline nature, such as lye, washing soda, ammonia, etc., are antidoted with vinegar or lemon juice, followed by soothing drinks or sweet oil.
A complete table of poisons and their antidotes will be found in the appendix.
Poison ivy, as soon as detected, should be treated as follows: Thoroughly scrub the affected part with tincture of green soap and hot water, which often prevents the trouble developing. Clean pieces of gauze may be wrung out of lime water and placed over the inflamed and much swollen surface, keeping them very wet. At night an ointment of zinc oxide may be applied over a painting of "black wash" (to be obtained at drug stores). Poison (trifoliolate, or three-leaved) ivy resembles Virginia Creeper, and all nurses and caretakers should be able to recognize it.
Another treatment for poison ivy which is said to be very efficient is as follows: Moisten a bit of cotton with a ten-percent solution of carbolic acid and apply to the affected area—then immediately (about one-half minute) wipe off this carbolic acid with another piece of cotton saturated with alcohol.
Matches, roach powders, fly poisons, washing fluids, lye, paris green, antiseptic tablets, and pieces of green paper, should all be kept out of the child's reach; and, in case of accidental swallowing of any of them, the physician should be sent for at once, and with the message "Come!" should be given the name of the poison swallowed—if it is known.
After the antidote is given, soothing drinks are usually administered, such as raw white of egg, milk, flaxseed tea, slippery elm, etc.
Complete rest in bed is always essential, and external heat is necessary for the body chills easily as the child grows weak.
Toothache may be temporarily relieved by applying an ice bag below the jaw, thus diminishing the flow of blood to the358 tooth, and a hot-water bottle to the cheek, which causes the skin vessels to fill with blood, thus relieving the tension in the vessels of the tooth.
If there is a cavity, a small piece of cotton moistened with oil of cloves and packed well into it may give much relief.
Children and adults should make a bi-annual pilgrimage to the dentist, who seeks out beginning cavities, early treatment of which will prevent these dreadful aches and later ill health.
Burns and scalds are not at all uncommon with children, whose eagerness to explore and desire to investigate often leads them into trouble.
1. The simple reddening of the skin—slight burns and sunburn—simply needs protecting oil, or equal parts of oil and lime water, and is to be covered with sterile gauze.
2. The burns which destroy the outer layer of the skin, producing a blister, are treated much as a wound would be treated. The blister, if larger than a half dollar, should be opened near the edge with a needle which has been passed through a flame. The serum should be pressed out and the parts protected by a piece of gutta-percha that has been disinfected with some antiseptic solution; this covering keeps the dressings from sticking, thus avoiding the destruction of the new-forming tissues.
3. When the tissues are injured in the more severe burns, the surrounding flesh is carefully disinfected with boracic-acid solution, and the same dressing applied as described for the "blister burns." Balsam Peru is a healing balm for burns of this classification.
If a child's clothes catch on fire he is instantly to be thrown on the floor and any heavy woolen fabric, such as a curtain, table spread, blanket, or rug, is to be thrown over him (beginning at the neck) and the flames thus smothered. The clothing is now cut off, and if more than one-third of the body is burned the child should be taken to the hospital for constant care; and if more than one-half of the body is injured recovery is doubtful. Great care should be taken in keeping the unburned portion of the body warm, as there is a great tendency for the359 child to become very cold as he weakens from both the nervous shock and from the absorption of toxins.
Acid chemical burns are treated with baking soda, except in the case of carbolic acid (misnamed), which is treated with alcohol; alkaline chemical burns are dressed in vinegar or lemon juice compresses.
Methods for restoring the drowned should be understood by every man, woman, and youth. These methods are more fully taken up in works devoted to emergencies and will not be discussed in detail at this time.
Consciousness is quickly restored to the fainting child by lowering the head—laying him flat on the floor—while an assistant raises the legs perpendicularly. Cold dashes of water may be slapped on the chest with a towel, while the face is bathed or sprinkled with cold water. Consciousness is usually quickly restored by the above suggestions, in connection with plenty of fresh air.
A sudden blow on the head occasionally results in a severe condition known as concussion of the brain. There is a partial or complete loss of consciousness lasting from a few moments to an hour or two. Pallor of the skin and a sense of bewilderment accompany concussion of the brain.
Rest, quiet, and darkness should prevail until the physician arrives and makes an examination. External heat to the extremities may be applied, but no stimulants are to be administered until so ordered by the physician.
It is wise to seek medical advice in the case of odd or unusual behavior after a fall on the head.
Most interesting is the study of the food as it passes through the processes of digestion, absorption, assimilation, and oxidation—all definite and important parts of the great cycle through which everything we eat passes on its way from the table to the tissues. Elimination is the last step in nutrition, and is the process by which the body rids itself of the broken down cells and other poisonous and useless wastes. These various phases of bodily nutrition may be expressed in a single term—metabolism.
What we eat and how much we eat must be carefully planned, for our body temple is really made of what we eat. If you were erecting a beautiful mansion you would not think of allowing cheap, trashy, and inferior building materials to enter into the construction of your home. Neither should you permit unfit and inferior materials to become a part of the daily dietary of your little boy or girl, thus to become a part of their bodily structure.
Following the process of digestion in the stomach and intestine, the nutritive food elements are absorbed through the wall of the bowel by the wonderfully adapted little villus, and distributed by various routes to the uttermost parts of the body. The sugars (all starches are changed into sugar) are carried in the portal blood stream to the liver, where they are actually stored away in the form of glycogen which, in a most intelligent manner, is dealt out to the body from hour to hour as it is needed for fuel. If all the sugar, after a hearty meal, were poured into the circulation at once, the blood stream would361 be overwhelmed and the kidneys would be forced to excrete it in the urine. This unnecessary waste is avoided by the liver's storing sugar after each meal and dealing it out to the body as required.
Likewise, the proteins also pass through the liver on their way to the body. Just what action the liver exerts upon proteins is not wholly known at the present writing. The digested fats are absorbed at once by the lacteals, the beginning of the intestinal lymphatic system, by which they are carried to the large veins at the root of the neck and there emptied into the blood stream. We have now traced our various food elements through the processes of digestion and absorption in the alimentary tract, some going through the liver, and others through the lymphatic system, until they circulate in the blood stream itself.
It is from these food substances, circulating in the blood stream, that the various cells of the body must assimilate into themselves such portions as they require for purposes of heat and energy and for the repair of their cell substance. This specialized work of cell assimilation converts the dissolved watery food in the blood into solid tissues, exactly reversing the process of digestion.
With a most profound intelligence, each of these body cells and tissues, bone and nerve fiber, muscle and organ, selects from the blood stream just its supply or portion of the food elements requisite to its upbuilding and maintenance. The mysteries of assimilation are effected by means of chemical substances called "enzymes," similar to those found in the digestive organs, but acting in an entirely different manner, in that they build up solids out of liquids instead of converting solids into liquids.
Metabolism consists of a twofold rôle—an upbuilding and a tearing down process. After the food is all digested, absorbed, and assimilated, having become a part of the bodily organ, bone, muscle, and nerve fiber, then begins the work of tearing it down—of liberating its heat and energy—to be followed by its362 elimination from the body through the sweat glands, uriniferous tubules of the kidneys, etc. The carbohydrates (starches and sugars), together with the fats, are completely burned up in the body and are then eliminated in the form of water (thrown off through the sweat) and carbonic acid gas given up by the lungs.
The proteins, or nitrogenous foods, are not so completely burned up in the body. The ashes which result from their combustion are not simple substances like the water and CO2 of the carbohydrates. This protein ash is represented by a number of complicated substances, some of which are solid (protein clinkers), which accumulate in the body and help to bring about many diseases, such as gout, headache, fatigue, biliousness, etc.
These protein ashes and clinkers are further acted upon—split up and sifted—by the liver, and are finally eliminated by the kidneys in the form of urea, uric acid, etc. The body being unable to store up protein, is often greatly embarrassed when one eats more of this substance than is daily required to replenish the waste of the body, for it must all be immediately split up in the system, and the over-abundant and irritating ashes must be carried off by the eliminating organs. Now, the overeating of sugars, starches, or fats, is not such a serious matter, as they may be stored in the liver and subsequently used; and even if they are eaten in excess of what the liver can care for they accumulate as fat or add extra fuel to the fires of the body, their ashes being carried off in the form of such harmless substances as water and carbon dioxide (CO2); but the overeating of protein substances is always a strain on the body and should be avoided.
There are seven distinct elements entering into the composition of human foods—protein, starch, sugar, fat, salts, cellulose, and water, not to mention enzymes, vitamines, and other little-known chemical principles. These elements are all variously concerned in the nourishment, energizing, and warming of the body.363
The proteins are the structure builders of the body. While starches, fats, and sugars may be compared to the coal that feeds the locomotive, the proteins represent the iron and steel that are used from time to time to repair the engine and replace its worn parts. The essential chemical difference between starch and protein is that the latter contains nitrogen and a small amount of sulphur and phosphorus. The most common forms in which protein is used for food are the glutens of the grains, the legumes, nuts, cheese, the white of egg, and lean meat.
The starches are by far the most abundant of all elements in human food. They enter largely into the composition of nearly all plants and seeds. Under the influence of the sunlight, the green-colored plants gather up the CO2 of the air and, with the water absorbed from the ground, build up starch. The plant takes all the carbon from which starch is made from the air, but while the atmosphere contains almost eighty per cent of nitrogen, the plant is unable to use it; it must secure its nitrogen from the decaying refuse of the soil. Thus the plant utilizes the waste products found in air and earth in the building of its food substances.
Starch exists in the form of small granules. Since each little starch granule is surrounded by a woody envelope of cellulose, it becomes necessary to cook all starches thoroughly in order to burst this cellulose envelope and thus enable the saliva to begin, and other secretions to continue, the work of digestion.
The sugar of fruits represents a form of food requiring practically no digestion; while the sugar found in beets, the cane plant, and the maple tree, must be acted upon by the digestive juices of the intestine before their absorption can take place. During the winter, the maple tree stores its carbohydrates in its roots in the form of starch. With the advent of spring Mother Nature begins the digestion of this starch—actually turns it into sugar—and in the form of the sweet sap it finds364 its way up into the tree trunk to be deposited in the leaves and bark in the form of cellulose, a process very similar to that performed by digestion in the human body, where starch by digestion is first turned into sugar, and afterwards deposited in another form in the liver and muscles.
Dextrine is a form of sugar resulting from thoroughly cooking or partially digesting starch. There are about twenty-five stages or forms of dextrine between raw starch and digested starch or fruit sugar. Dextrine is found in the brown-colored portions of well-toasted bread.
Fat is a combination of glycerine and certain fatty acids. As a food, it is derived from both the animal and the vegetable kingdom. Animal fat consists of lard, suet, fat meat, etc., while fat of animal origin is represented by cream, butter, and the yolks of eggs. The vegetable fats are found in nuts, especially the pecan, cocoanut, Brazil, and pine nuts; also in the grains, particularly oats and corn. The peanut also contains a considerable amount of fat. Of the fruits, the banana and strawberry contain a trace of fat, while the olive is the only fruit rich in fat.
As a food, fat is used in three forms. The emulsified form is represented by cream, olive oil, and nuts. When the tiny globules of fat, which are each surrounded by a little film of casein, are crushed—united into a solid mass—we have a free fat. This form is represented by butter and other animal fats. Another form is fried fat—fat which has been chemically changed by heat with the development of certain irritating acids.
The mineral elements comprise but a small part of human food as regards weight, but they are extremely important to the health of the child as well as the adult. As found in the food, they are not in the form of mineral salts, like common table salt. The salts of food are living salts, organic or organized salts, such as are found in the growing plant. These salts365 are of great value to the various fluids of the body, and also as stimulants to nerve action, but more particularly in the work of building up the bones.
Salts are found largely in the cereals. A small amount is also found in vegetables, particularly the potato, as well as in most fruits.
Cellulose represents the great bulk of all vegetables and fruits. It is digested by most animals, but in man it is digested only to the extent of about thirty per cent. The presence of a large amount of cellulose in the food enables us often to satisfy the appetite without injury from overeating. It serves to give bulk to the food, and thereby possibly acts as a preventive to constipation.
Water fills an important place in the nutrition of the body. The food changes in connection with digestion, assimilation, and elimination, can take place only in the presence of water. Water constitutes from fifteen to ninety-five per cent of the various foods. The watery juices of vegetables and fruits consist largely of pure, distilled water, in which fruit sugar is dissolved, with added flavoring substances. Water is absolutely essential to the performance of every vital function connected with human metabolism.
The source of heat in the animal body was the subject of much superstitious speculation on the part of ancient scientists. It is now known that animal heat is derived from the food we eat by means of a peculiar process of vital oxidation—effected in the presence of oxygen—by the action of water and enzymes upon the food elements absorbed by the living cell. This process of oxidation liberates the heat and energy stored by the sun in the food, and thus the body is kept warm by this constant combustion of the digested foodstuffs. The starches and sugars, together with the fats, represent food elements which366 serve as the body's fuel. By this means we are able to maintain a constant body temperature of almost one hundred degrees.
The average human body produces enough heat every hour to raise two and one-half pounds of water from the freezing point to the boiling point. This is equivalent to boiling about seven gallons of ice-water every twenty-four hours. Differently expressed, the body gives off each hour the same amount of heat as a foot and a half of two-inch steam coil. This is the same amount of heat which would be produced by burning about two-thirds of a pound of coal.
Expressed in terms of English weight, the fuel value of the three different food elements would be:
| 1 ounce of carbohydrates | 127.5 calories |
| 1 ounce of proteins | 127.5 " |
| 1 ounce of fat | 289.2 " |
It will be observed that fat contains more than twice as much heat as the carbohydrates. This is due to the fact that fat contains more carbon than either starch or sugar. Next to fats, starches and sugars are the most important fuel elements. Protein is a very extravagant form of food for fuel purposes. Proteins are the most expensive elements of human food; they are incompletely burned in the body, and inasmuch as they leave behind distressing and disease-producing ashes, it is clearly evident that only sufficient amount of proteins should be eaten each day to supply the demand of the body for repairs. We should depend more largely upon the carbohydrates and fats for heat and energy.
A large part of our food is required to furnish heat to take the place of that lost by radiation from the skin, and this is why children require more food than adults—they have a larger skin surface in proportion to their weight, and therefore lose more heat by radiation, and it is for this reason that the food for the growing child must be wisely and carefully selected.367
Breakfast, 7-8 a. m.: Fruit; cooked or toasted cereal served with thin cream; a soft boiled or coddled egg; bread (two or more days old) and butter; plenty of milk.
Dinner, 12-1: Soups; creamed vegetables—tomato, corn, peas, and celery; any two of potatoes—creamed, mashed, or baked—carrots, beets, spinach, peas, cornlet, squash, cauliflower, asparagus tips, string beans; protein dish—the puree of dried beans, peas, or lentils; macaroni or carefully selected meats; dessert—apples, baked or sauce—or other fruits, junket, custard, milk.
Supper, 5-6 p. m.: Fruit, bread (bran bread if constipated); milk; porridge, with rich milk or milk toast; sweetened graham crackers.
Protein Dishes: Purees of dried peas; lentils; beans; macaroni; eggs—soft boiled, poached, scrambled, or omelette; meats—steak, chops, chicken, turkey, broiled fish.
Cereals: All the toasted-flake foods; toasted and not too fresh bread, including both graham and bran; hominy; corn meal; oatmeal; farina; rice; barley; tapioca; sago, etc.
Soups: Creamed vegetable soups of all kinds and broths.
Vegetables: Potatoes; all the small green vegetables; lettuce; stewed celery; beets; squash; cauliflower, etc.
Fruits: All, if stewed or baked. Raw fruits—pears, peaches, ripe apples, berries, oranges, persimmons, grape-pulp without seeds, etc.
Desserts: Custard; jellos; junkets; home-made ice cream; sponge cake; baked fruits with whipped cream, etc.
1. Doughy breads, griddle cakes, insides of muffins, hot biscuits, etc.
2. Fried meats, such as sausage, oysters, pork, ham, veal, salt fish, corned beef, dried beef, etc.
3. Foods that are hot when they are cold—such as catsup, horse radish, mustard, highly spiced pickles, sauces, etc.368
4. Rich pastries, puddings, unripe fruit, salted peanuts, and highly concocted dishes.
5. Certain salads, containing coarse but easily swallowed foods, with highly seasoned sauces.
6. Tea, coffee, and all alcoholic beverages.
7. Soft candies, chocolate creams, bon-bons, patties, etc.
Average normal children crave sweets, and since their normal food is about seven per cent sugar it is not to be wondered at. There are many forms of pure, hard candies which may be taken by the three-year-old child. They are stick candy, fruit tablets, sunshine candies, and other varieties which may be sucked.
All soft candies, such as chocolate creams, bon-bons, patties, etc., are to be avoided. Hard candies, taken along with the desserts at meal time, in no wise injure the normal stomach of the healthy child.
The other members of the family should set a correct example by sucking the hard candies rather than chewing them; for if the hard candies are allowed to dissolve slowly in the mouth they produce a weak solution of sugar, which does not interfere with digestion as do the strong and concentrated sugar solutions which result from chewing chocolate creams, bon-bons, etc.
Candy, cookies, sandwiches, or bits of cake should never be allowed between the meals.
Children who do not eat well at the breakfast table, if given a "piece" at 10 a. m., will not be ready for the 12 o'clock meal; and then another "piece" at 2 p. m. interferes with the normal appetite at 6 p. m. Digestion is disturbed, the nervous system irritated, and a "puny child" is often the result.
Bring the three-or-four-year-old to a well-selected breakfast some time between 7 and 8 a. m. Then nothing—absolutely nothing—but water must pass the lips between that breakfast hour and the 12 o'clock meal, which should be a good one. Then the interval until 5 or 6 p. m. is passed in the same manner. At the evening meal the appetite is again whetted: and a good appetite always means good gastric juice to digest the369 meal. And so, good mother, guard carefully the interval between meals if you would have good digestion and good health for the little folks.
The following table, taken from The Science of Living,[4] shows the minimum of calories or food units required by boys from five to fourteen years of age and girls from five to twelve:
| Age Years |
Height in inches |
Weight in Pounds |
Skin Surface in Sq. Ft. |
Daily Calories or Food Units |
| 5 | 41.57 | 41.09 | 7.9 | 816.2 |
| 6 | 43.75 | 45.17 | 8.3 | 855.9 |
| 7 | 45.74 | 49.07 | 8.8 | 912.4 |
| 8 | 47.76 | 53.92 | 9.4 | 981.1 |
| 9 | 49.69 | 59.23 | 9.9 | 1034.7 |
| 10 | 51.58 | 65.30 | 10.5 | 1117.5 |
| 11 | 53.33 | 70.18 | 11.0 | 1178.2 |
| 12 | 55.11 | 76.92 | 11.6 | 1254.8 |
| 13 | 57.21 | 84.85 | 12.4 | 1352.6 |
| 14 | 59.88 | 94.91 | 13.4 | 1471.3 |
| Age Years |
Height in inches |
Weight in Pounds |
Skin Surface in Sq. Ft. |
Daily Calories or Food Units |
| 5 | 41.29 | 39.66 | 7.7 | 784.5 |
| 6 | 43.35 | 43.28 | 8.1 | 831.9 |
| 7 | 45.52 | 47.46 | 8.5 | 881.7 |
| 8 | 47.58 | 52.04 | 9.2 | 957.1 |
| 9 | 49.37 | 57.07 | 9.7 | 1018.5 |
| 10 | 51.34 | 62.35 | 10.2 | 1081.0 |
| 11 | 53.42 | 68.84 | 10.7 | 1148.5 |
| 12 | 55.88 | 78.31 | 11.8 | 1276.8 |
4 Sadler, William S., The Science of Living; or, The Art of Keeping Well. A. C. McClurg & Co.
Because of her versatile adaptability to the management of details, woman, all through the ages, has willingly and happily sacrificed herself upon the altar of service. It is not in the province of this chapter to go into the details of the tribal life of the early hordes and clans that came from the north and from the east to establish civilization in the cities of Rome and Britain—space forbids. In this chapter we wish to hold up a picture to the mother, a picture which may speak volumes to her soul; one which perhaps she may ruthlessly throw away—nevertheless, we propose to exhibit it.
A newspaper woman in my office recently told me a story of a mother who finished her high-school education, took some work in a university, and who yielded to the earnest pleas of her lover-classmate through grammar school, high school and college—and married him. To this happy family there came a number of beautiful children. The mother willingly, lovingly, cared for them during their helpless infancy—made their clothes, managed their meals, opened the door for them as they came home from school, met them with a cheery story, listened to their problems, helped them with their lessons—but all through it, first, last and all the time, she also managed the entire home. She dusted the furniture, changed the curtains, looked after the linen, mended the clothes, and even pressed the trousers of her "rapidly rising" husband that he might go out into his "club life" and enjoy the evenings with his associates. The duties of the day so wearied her, and the night vigils with the sick child,—looking after the little coughs, the371 uncovered shoulders, getting the drinks of water and performing a dozen other details—that she was too weary to accompany her husband to the dance, to the theater, to the social gathering or to ladies' night at the club; and so, in the course of a dozen years, the mother had grown old, and quite naturally she had grown "home centered." Her world's horizon was the walls of her home. She was happy and quite contented in her children's smiles, in the cheery "how do you do" of her husband, in the fact that that gravy was good or that steak was fried to the king's taste.
She was happy and contented until one day when the awakening blow came. In the attic she and her thirteen-year-old son, who was just entering high school, were looking through an old chest when she drew forth some examination reports and some old school cards—holding them up side by side. One set of the cards bore the father's name and the other set the mother's maiden name. In great surprise the boy exclaimed, "Why, mother, I never knew you studied algebra and Latin; why, mother, I never knew you were educated." Her eyes were immediately opened, the scales fell off, she was awakened to the fact that her own son was coming to regard his mother as somewhat inferior, in intellectual attainments, to the father—that she was considered in that home as a mere domestic. True, the steak had been broiled well, the pudding was exquisite, the children's clothes were always in order, the husband's trousers were always beautifully pressed, his ties were cleaned as well as a cleaner could clean them; but where did she stand in her boy's mind and where was she in her husband's mind?
"Do you notice how trim and nice Mrs. Smith always looks? Her clothes are always in the latest style, and she combs her hair so becomingly." Such remarks as this from the well-meaning husband cut keenly, and it is well that they do, for often it is only such remarks that wake up our "home mother."
Dear reader, I want you to ponder this story. I wish to say to the mother who has started out upon a career in life, who has prepared herself for teaching school, for a business career, for story writing, for millinery, for lecturing, or has perhaps gradu372ated in a domestic science course, that she makes the mistake of her life in settling down, just because she has taken another's name, to be perfectly satisfied with becoming the household domestic, the household mender, the household cook.
I have in my acquaintance scores of mothers in the professions, newspaper women, women who have carved out brilliant careers for themselves, women who have taught school for twenty years while their children have been growing up, women physicians who have risen in the esteem of all their professional brothers and sisters, women who have conducted cooking schools, who have occupied positions of trust in hospitals and in every walk of life, and who have successfully reared children at the same time.
You will pardon me for being personal when I say that since our own little fellow was six weeks old his clothes have been washed and mended and his food has been prepared by earnest and honest women who had not fitted themselves for the career which this boy's mother had chosen. His mother went to her office, cared for her patients, kept up by the side of her husband in the battle of life. All the time there was a woman at home just devoted to that little fellow.
A newspaper woman recently told me her story—a story which should impress everyone of my readers as it did myself, and she, like many other mothers in the professions, leaves her home as the little fellow goes to school. His hands have been washed, his bowels have moved, his hair has been combed, his breakfast has been eaten by the side of his mother—she has directed it all. He goes forth to the schoolroom and she goes forth to her profession. All through the day she lovingly keeps in mind these children that are growing up. She works the harder, real love entering into everything she does, because she is not merely earning the bread that goes into their mouths, but is forming a character not only for herself but, because of her broadened horizon, is instilling into their little minds the possibilities of their own career, their own opportunity to enter into the world's work as real world workers.373
I contend that the mother in a profession has many blessings that the mother who remains at home never has. The mother who remains at home has a viewpoint that is often quite likely, wholly unconsciously, of course, to become small, to become narrow, to become focused upon small details; on the other hand, the mother whose mind and whose heart are so full of the affairs of the office, of the newspaper article she has just written, or the lecture she has just given or is about to give, or the meeting that she is to preside over, is quite likely to become somewhat irritated sometimes if the little fellow doesn't stand quietly to have his hair combed, she is quite likely to "feel rushed;" but under all circumstances, dear reader, whether this mother be a home mother or in a profession, never, never must she allow mental panic to seize her. Ever must we keep in mind that these little ones are just children—children that are still in the developmental stage.
And now for the home mother. I believe it is necessary and of paramount importance that she get away from her children (if possible) several hours each day; that she provide for them a caretaker who can relieve the children of her or relieve her of the children, whichever way you may look at it, for we are inclined to think that the children often tire of the mother just about as often as the mother tires of the children. I would have the woman who remains at home, whose husband is able to provide outside help for the heavy work of the house, enter into some uplifting neighborhood work, social settlement work, church work, wholesome club work—anything but bridge and whist and gambling games. I would have them bring into the nursery a woman who is cheery, who is capable of teaching games, of entertaining and amusing these little folks under their own roof.
The woman who has graduated from high school, who has a diploma to teach, I would have take a school or, at least, do substitute work. She will be happier—far happier—continuing along the lines for which she has prepared herself, even if all the money she earns be used to pay the help. Some374 women are especially fitted for the important work of mother and homemaker, and such wives will find for themselves a worthy career in the home and its neighborhood activities. Each woman must find a field of action suited to her own temperament, education, experience, talents, and opportunities.
For a caretaker, the professional or business woman should not select an ignorant servant girl; that would be a great mistake—a crime—a violation of the law that should govern the training of these little people who have come to us to be reared and cared for and fitted to occupy their place among the world's workers. As a rule, one soul does not possess the qualifications for scrubbing and laundry work and also the firm but gentle ministering qualifications necessary for a successful caretaker. They do not combine as a rule. It has been my experience, as a mother with a profession, and that of many others of my acquaintances, that an art student or a music student makes a splendid caretaker. There are hundreds and hundreds of genteel women, with winning manners and beautiful dispositions, who may be obtained to sew on the buttons, wash the faces, and change the clothes of our darlings while we are carrying forward in the world the great work for which we have fitted ourselves during the long struggles of our teens and early twenties.
The young woman who is brought in to care for the child should be above the usual "servant" class. She must eat in our dining-room, she should be welcome in the living-room or sun parlor, and be treated as a respected member of the family. Her salary is usually not large for she realizes that she is given something in that home—something that money cannot buy.
Now this young woman (the caretaker) wants to hold her position, and so she is very anxious to carry out in detail the laws and rules that are laid down by the mother. Mother can keep abreast with the world, mother has time to read periodicals that keep her in touch with the great, wide, pulsating375 affairs of life. She is able to meet more women worth while, and with her husband attend lectures, musicals, theaters, and other places for intellectual culture.
Anyone of my readers need not look four blocks from her home to find a mother who is run down at the heel, whose dresses are calico, whose hat is five or six years old, whose black silk dress (the only one she ever had) is worn shiny or threadbare, who works and saves every penny that she can that her children may look well; and, even when the husband does invite her to go out with him, he will often be confronted with this remark: "John, I would like to go, but really my clothes are a little bit shabby." The world is just full of such women, with their very hearts being eaten out of them for the want of a beautiful gown, a beautiful hat or a pretty pair of evening shoes, and they might have them every one if they would be willing to allow the duties of the household to be presided over by a woman that cannot do the things the mother can do, while she goes out and accrues a number of dollars each week which will more than provide for the things that her soul desires so that she may go well dressed by the side of her husband in quest of that very necessary intellectual culture and social diversion.
The wife of a prominent judge, in my office just this week, said to me that she believed that most of our social and domestic uneasiness was due to the fact that fathers and mothers and children went out together so seldom. The father goes to his club, the children go to their little gatherings, and mother usually stays at home; although of late, she is beginning to realize the value of the women's clubs.
The caretaker should not be too old. It is a very great blessing if there is an older sister in the family who can come in and assist with this work, or if there is an aunt. If one is to be selected from the open market, then we suggest a woman in her late teens or early twenties whose heart is full of play, whose face is sunny, and who is young enough to appreciate and like the becomingness of youthful dress. It is376 needless to say she should be free from tuberculosis and other diseases. She should be trustworthy enough not to administer soothing syrups because the children won't sleep, or to give candy when mother has forbidden her, or to teach the children bad habits of any sort.
It is impossible to exercise too much care in the selection of this substitute mother, and when you do find one it is often wise not to keep her too long. A year or so is plenty long enough for any person to be with our children. It is only necessary for anyone to walk out into the public parks and casually listen to the conversations of many of the "chewing-gum caretakers" to discover with what carelessness some people select caretakers for their children. The language they use is not only ungrammatical but oftentimes both slangy and profane. The flirtations carried on with many of the park policemen and bystanders lead us to feel that many people arrive at the idea that their little folks "will grow up some way." If the caretaker is a student, a young woman of culture, and is kept with the family, she will be found to be more circumspect and dependable. Her gentleman friend, if she has one, should be allowed to come to the home. She does not have to meet him out in the park any more than a sister would have to go away from home to meet a friend; and, to my mind, everything centers around the viewpoint of the mother as she selects this caretaker, for if she is her social equal it puts her in a different place entirely to the well-meaning but ignorant servant girl to whose care is often intrusted the lives of the little people.
There are a number of hints we wish to bring together in this chapter for the mother to suggest to the caretaker. For instance, here is a group that one author gives us:
He is dry.
He is healthy.
His food is right.
377He has sleep enough.
His meals are on time.
He is dressed properly.
He is bathed regularly.
His habits are regular.
His bowels move regularly.
He has fresh air day and night.
He is not dosed with patent medicines.
He is not excited by frequent handling.
He is not annoyed by flies or other insects.
Candy.
Pacifiers.
Thumb-sucking.
Soothing syrups.
Patent medicines.
Waterproof diapers.
Moving picture shows.
Sucking on empty bottles.
Being kissed on the mouth.
Play of any sort after feeding.
Sleeping in bed with the mother.
Whiskey or gin for supposed colic.
Sneezing or coughing in the face.
Irregular or too frequent feedings.
Sleeping on the mother's breast while nursing.
Spitting on handkerchief to remove dirt from baby's face.
Allowing a person with a cough or a cold to hold the baby.
Violent rocking, bouncing, and rollicking play at any time.
Dirty playthings, dirty nipples, dirty bottles, dirty floors.
Allowing any person with tuberculosis to take care of the baby.
Testing the temperature of the baby's milk by taking the nipple in the mouth.
Keep baby out of dust.
378Don't cover his face.
Don't rock him to sleep.
Keep baby away from crowds and sick people.
Don't neglect a sore throat or a running ear.
His health, growth, and happiness depend largely upon you.
Cats and dogs have no place about a baby. They carry disease.
The baby is not a toy or a plaything, but a great responsibility.
Don't wipe out baby's mouth. It tends to cause ulcers and thrush.
There are a few bad habits which older children fall into such as lip-sucking or thumb-sucking or finger-sucking which not only narrow and deform the upper jaw, but likewise deform the hand itself. They should be stopped at the earliest opportunity by pinning the sleeve to the bedding or putting mittens on the hand or putting a slight splint on the anterior bend of the elbow. Some children suck their handkerchiefs, or bite holes in their aprons and neckties.
Children often bite their finger nails, and a habit of this kind fully developed during early childhood often remains with them throughout life; whenever a nervous spell seizes them they instantly begin to bite their finger nails. Other people pick their nose when nervous, so during very early childhood these habits should be discouraged. One mother helped her little son by beautifully manicuring his nails for him each week. Another child was cured by old-fashioned spanking. The finger tips may be painted with tincture of aloes, or dipping the tips of the fingers in strong quinine water will sometimes help. I know of nothing better for the adolescent child than to teach him how properly to manicure his own nails. Another bad habit that children often get into is stooping or allowing the shoulders to become rounded. Shoulder braces are not indicated in these cases. The children should be allowed to enter the gymnasium or the father should take off his coat and vest and go through gymnasium stunts with the boy. The mother can do the same for the girl. It is often the case that round-shouldered379 children are near sighted. The child really has to stoop to see things. When a child holds his head to one side constantly on looking at objects, astigmatism, an error of eyesight, is usually indicated. An eye specialist should be consulted, the eyes examined, and properly fitted eye glasses should be worn.
Just as early as possible in the life of the little child he should be taught to blow his nose, to spit out the coughed up mucus from his lungs, to hold out his tongue for inspection and to allow his throat to be examined. He should be taught to gargle, and to regard the physician as one of his best friends. Attention to these minor accomplishments will make it very easy indeed for the physician in case of illness.
A child is the most imitative creature in the world. Before he is out of pinafores he tries to talk and act just like his elders. It is because of this inherent tendency to say and do those very things which he hears others say and do, that, if faith-thoughts are early and constantly suggested to the unfolding mind of the child they will assist greatly in evolving a character of joy, confidence, and courage. On the other hand, if fear-thoughts are continuously sown in the young mind they will eventually distort the emotions, deform the conceptions, and wholly demoralize the health and life activities of the growing child. Within the limitations of the possibilities of hereditary endowment, and in view of this wonderful imitative nature, we are able to make of a child almost anything we desire; not "an angel," in the ordinary acceptation of the term, but a child who knows his place and possesses the power of normal self-control.
From two to six years of age, when the imagination is most plastic and vivid, when the child's imitative instinct is so unconsciously automatic, is the most effective and opportune time to initiate good habits and lay the foundations for the later development of a strong and noble character. "Baby's skies are Mamma's eyes" is just as true as it is poetical. While a tired and worn-out mother, exhausted by a multitude of harrassing household cares, may be pardoned for her occasional irritability, nevertheless the little one unconsciously partakes of her spirit. When the mother is happy the child is happy. When Mother is sick and nervous the child is impatient and irritable.
It is unfortunate that this very time of a child's life, when381 we can do practically anything we choose with him, is the very time when so many parents fill the child's mind with the unhealthful fear-thoughts. "The bogie man'll get you if you don't mind Mamma," or, "I'll get the black man to cut your ears off," or, "the chimney sweep is around the corner to take bad little boys," are familiar threats which are so frequently made to the little folks. These efforts to terrorize the young child into obedience never fail to distort the mind, warp the affections, and, more or less permanently, derange the entire nervous system. The arousal of fear-thoughts and fearful emotions in the mind of the growing child is very often such a psychologic and a physiologic shock to the child that the results are sometimes not wholly eradicated in an entire lifetime.
Just see how far we carry this unwholesome introduction of fear-thoughts—even to the Almighty. Thousands of us remember being told as a child that "God don't like naughty boys," or, "God will send the bad man to get you if you don't be good." Thus, early in life, an unwholesome fear of the Supreme Being is sown in the mind of the child, and, as time passes, these false fears grow and come so to possess the mind and control the emotions that in adult life this early teaching comes to mold the character and shape the religious beliefs of the individual.
To the child who has been reared to dread God, who has come to look upon the Creator as an ever present "threat," how is it possible to convey the beautiful teaching of His fatherhood?
How frequently some unusual noise leads a parent to say: "Keep still! What was that? Did you hear that noise?" The little folks of the family are startled, their eyes grow large and their faces pale, while they cling to the frightened mother. Of course, investigation usually shows that the strange and alarming noise was merely the slamming of a cellar door, the rattling of a curtain in the wind, some one walking about downstairs, or the action of the new furnace regulator in the basement. But meantime the harm is done to the children—fear, the worst enemy of childhood, has been unconsciously planted in the mind by the thoughtless and nervous parent.382
Consider for a moment the thousands of children who are early taught an abnormal fear of the dark. Even when the child is absolutely free from such a fear, when sent into a dark room some member of the family will thoughtlessly remark, "Do you think it is quite right to send that child into that dark room? Suppose something should happen." The child quickly catches the suggestion that something is supposed to be or happen in the dark, and in his mind is sown the seed of fear.
When our boy was about two years old he was carried one night to the window by a caretaker, and as they looked out into the darkness the young woman said, "Boo! dark!" The little fellow shuddered, drew back and repeated, "Boo! dark! Boo! dark!"
That night, as was our custom after the evening story, we tucked him in his little bed, turned out the light, and saying, "Sweet dreams, Darling," closed the door. Imagine our surprise to hear, "Mamma, Mamma, Willie 'fraid of dark, Willie 'fraid of dark," and it was with difficulty that he was induced to go to sleep in the dark. Immediate inquiry revealed the occasion of his fears, and the next night we set about to eradicate the fear of darkness from the little fellow's mind.
For ten successive nights we took his hand, and, leading him into a dark room, said, "Nice dark, restful dark; we go to sleep in the dark; we're not afraid of the dark, no." Each night, save one, we were met with, "No, no, naughty dark. Willie 'fraid of dark." On the tenth night as we entered the room as usual, repeating, "Nice dark, restful dark; we go to sleep in the dark; we're not afraid of the dark, no," his little mind responded. Suggestion had at last routed fear and given birth to faith. We had won! But it had taken ten nights of constant work to undo one moment's work of a thoughtless girl. Every night since he has gone to sleep in the dark without a murmur.
Threats only show weakness on the part of the disciplinarian. Most school teachers early learn the folly of making threats. When I was teaching school I recall that a number of slate pen383cils had been dropped on the floor one afternoon. Thoughtlessly I threatened, "Now the next child that drops a pencil will remain after school and receive punishment!" My fate! The weakest, most delicate girl in the room was the next to drop her pencil, and she was a pupil with a perfect record in deportment. The reader can imagine my embarrassment. I had threatened punishment, and so had to get out of the predicament as best I could. This experience effectually cured me of making such foolish threats.
Most of us live to regret the threats we make. "Your father will thrash you when he comes home tonight," or, "You'd better not let your father see you doing that," or, "You wouldn't behave that way if your father was here," etc., are common threats which we hear directed at headstrong and willful boys. What is the result? Do such threats cause the love of the child for his father to increase? They make the child actually afraid of his father.
"I'll 'bust' your brains out," said a four-year-old to his pet lion, because it wouldn't stand up. Now it should be remembered that these things do not originate in the minds of the boy and girl. They only repeat the things they hear others say. It betrays both cowardice and ignorance to undertake to secure obedience by such threats as "I will box your ears if you don't mind," etc.
Obedience that is worth anything at all is only secured by suggestion and love, never by promises of reward or threats of punishment.
Recently we overheard a little fellow say, "Father says I'm the only coward in the whole family." Looking him straight in the face we said to him: "You're not a coward. Such a fine boy as you couldn't possibly be a coward." The boy was greatly amazed, and, as we left him, he was saying over to himself, "I'm not a coward. She said I'm not a coward," finally adding, "She said I couldn't be a coward." This one thought, repeated to him several times and turned over and over in his mind, eventually overthrew the false fears instilled by his father.384
A short time ago the daily papers contained the story of the ten-year-old son of a New York business man who drew his few dollars from the savings bank, boarded a train for Chicago, and, after three days of amusement and loneliness, his money all gone, was found in a hotel bitterly weeping. His identity was revealed, the parents were notified at once, and the boy was sent on the first train back to his home. On the way to the station he sobbed out through his tears, "Well, my brother can't call me a coward any more, anyway." Who knows but that this everlasting taunting of the child with the accusation of being a baby or being a coward has much to do with many such escapades and other daring exploits on the part of the juveniles who are chafed by such unjust insinuations? Those of us who are acquainted with the vice and crime of a great city can imagine just what might have happened if this boy had been a little older, if his heredity had not been so good, if his money hadn't run out, if he had been able to remain in the big city long enough to make undesirable acquaintances.
Many criminals have confessed behind prison bars that when they were children they were called cowards. After a while they actually came to believe that they were cowards, and in their efforts to acquire courage and demonstrate their bravery they were led to desperate and even criminal acts. They prowled around the dark alleys just to convince themselves that they were not afraid, that they were not cowards, and there they made the acquaintance of the criminals who led them into new and dangerous paths. Even if a child enters this world handicapped by heredity, let us not lessen his chances of success by adverse suggestion.
Faith-thoughts, thoughts of bravery and of courage, may just as easily be instilled into the mind of the normal child as thoughts of fear and cowardice. A child should never have suggested to him that he is afraid. He should be constantly assured that he is brave, loyal, and fearless. The daily repetition of these suggestions will contribute much to the actual acquirement of the very traits of character that are thus suggested. This does not mean that a child should not be taught caution and forethought.385
Parents do not begin to realize how fearfully dangerous is this habit of constantly reiterated negative suggestion. Let me illustrate by an actual incident: A beautiful girl in a near-by state grew up quietly in the little village until she was eighteen years of age, when suddenly she decided to run away from home, declaring she was old enough to do as she pleased. She confided in one of her girl friends that she was going to Chicago, and had made all arrangements to lose herself in the "redlight" district. All that this girl friend said had not the slightest influence. As the train bore her away to the city and to ruin, a social worker in Chicago was wired to meet her at a suburban station. The girl was met, taken from the train and whisked in a cab to the home of a Christian woman. So possessed was this girl with the idea of throwing herself away that the captain of police was asked to talk to her; but the combined efforts of the police captain, a magistrate, and several Christian people could not persuade her to recall her threat. She declared she would kill herself if her parents were notified. This siege lasted for ten days. Then she finally broke down, saying: "I simply can't help it. All my life my mother has told me that I was going to turn out bad. No matter what would happen at home, if I broke a dish or went out with the young people and remained away ten minutes later than I was told to, it would always be thrown up to me. 'Oh, some day you'll turn out bad.' I have heard it until I am sick of it, and something within seems to push me on and on, telling me I must turn out bad."
Of course the girl was persuaded to believe that these were only fear-thoughts; that she was a beautiful, virtuous girl, that she simply had received the wrong training, that she couldn't possibly turn out bad. She was thus saved by the sympathy and advice of understanding friends, was subsequently married and is today the mother of a splendid boy.
Here is another story which illustrates what healthy faith-thought will do. A young man was not long ago selected for386 the highest position within the gift of a large religious organization. When he was a lad his parents held this thought constantly before his mind: "David, if you will be a good boy, if you will do what is right, you may some day be President of the General Assembly." He became a minister of the Gospel, a very successful one, and subsequently married a young woman who was also much interested in religious work. She continued to encourage him in this ambition, saying: "David, preach the best sermons you can; make an effort to bring many souls to Christ, and some day I believe you will be President of the General Assembly." The man presided over the General Assembly of his denomination, not one term, but term after term. He kept his eye long fixed on that particular aim, and by faith he won it.
To see how powerful suggestion may be in a child's life take this incident that every parent knows: The little one trips and tumbles. Mamma says, "Oh, did you fall? Well, never mind; come here, I'll kiss it. There, now it's well." Immediately the child goes back to his play perfectly happy. One little fellow was taught that when he fell he should get up at once, rub the bump, and say, "That didn't hurt." All through his career the bumps and the hardships of life were met with the same pluck. On the other hand, a thoughtless caretaker will excitedly jump and catch up the slightly injured child, coddle it, rock it, pet it—and the crying continues indefinitely. This early training in meeting minor hurts and obstacles lasts throughout the lifetime. Pluck and grit are lacking. The behavior of the man in the face of difficulties is foreshadowed by the attitude of the child toward his petty trials and bumps.
Successful child training follows in the path of positive suggestion. Impatient words and careless threats of punishment can only contribute to the wrong training of the young mind.
When is the best time to suggest to the child? Catch the little fellow when he is happiest, when he is overjoyed and filled with glee; for it is at such times that the suggestions offered will meet with the least resistance.387
Teach the children through the spirit of play and through the medium of the story. The boy or girl in the story always can have a clean face, always close the doors quietly, and otherwise so conduct himself or herself as to constitute a powerful positive suggestion for good. The story-child always says, "All right, Papa," "All right, Mamma," when corrected.
The "going-to-bed time" is the time par excellence for suggestion in early childhood. After the play time, the study time, and the evening story, when all is quiet, in the peacefulness of the darkness, while you are seated in a low chair close beside the little bed, with your hand in his, repeat over and over again the positive suggestions which you desire to take root in the mind and bear fruit in the character. Again and again tell the little fellow that he is the noblest and bravest of boys, that he loves truth and hates deceit. No matter what disturbs him, if it is the lessons at school or a wrong habit, first think out exactly what you desire him to be or to do, and firmly, but quietly, tell it over and over to him.
As a concrete example: Suppose Henry, at three-and-a-half years of age has to be coaxed or almost forced to eat. Say to him: "Now, Henry, you are a good little boy. Papa and mamma love you dearly. If you are going to grow up to be a big man you must not forget to eat; so tomorrow when you go down to the table you will eat everything mamma or nurse puts before you. It won't be necessary for papa to feed you at all; you will eat the potatoes, the gravy, the toast, and the cereal, and drink your milk. You will make mamma very happy, and papa will be proud of you; and then after dinner we will have a good romp, and you will soon grow up to be big enough to have a velocipede and a watch." After two or three evenings of this suggestion you will be surprised to see there is a great difference in his eating.
Take the timid little girl who is unable to recite well at school, who is shy, and has great difficulty with her lessons. At the going-to-sleep time sit by the side of her bed and tell her that tomorrow she will have her lessons better, that she will388 not any more be afraid, that she will get up and recite without the least fear in her heart. By constantly repeating these suggestions she will be given confidence, and in most cases it will result in effecting the deliverance of the child from her bondage to fear. Never tell her that she is shy or that she cannot do things. Constantly tell her that she is a successful girl with a strong character, and that she is going to make a very useful and courageous woman. Hold high aims and ideals before her. Suggestion cannot atone for all the defects of character which may be inherited, but it can do much to help such unfortunate little ones gracefully bear their burdens.
Never tell children that you suspect they are dishonest or untruthful. Be very slow to accuse and suspect them of falsehood or theft. Tell them over and over again they are the best boys and girls in the world; that they are going to make the noblest of men and women; that they love honesty and truth. Even when you discover them in minor faults do not make the mistake of unduly magnifying and emphasizing the error. As soon as possible direct the thoughts and attention of the wrongdoer away from his error, and focus his thoughts and attention on the high goal you expect him to reach. This will not be construed as doing away with proper punishment for persistent faults after the more ideal methods seem to have failed.
A patient recently called us to see her little girl, and as we made ready to make the examination the mother said: "Now, Mary, stop your playing and come and be undressed and let the doctor look at you."
"I don't want to stop playing," murmured Mary.
"But you must come. You know you don't feel well at all, your cheeks are so red. Now swallow and see if it don't hurt. Now try again. I know you don't feel well." By the time we had begun our examination Mary began to succumb to her mother's suggestions, and began to feel a trifle indisposed. She was being made temporarily ill by the unwise and unfortunate suggestions of the overanxious mother. The ex389amination revealed that there was nothing whatever the matter with her.
Let us get the truth firmly into our minds as parents that it is just about as easy to form a good habit as a bad habit, just about as easy to acquire helpful, happy thoughts as those that are injurious; and we can do it, if we will but see to it that our children early form correct and proper habits of thinking and acting. While the children are taught proper respect for authority, let fear be an unknown word to them. Don't let a thought of the fear of insanity, of haunted houses, of drafts, of this and of that enter into your home. Instead, live in the glorious sunshine of strong, healthy, faith-thought, and a supreme happiness will come into your life, and you will give a legacy to your children for which they will "rise up and call you blessed."
The love of mother and sister can naturally and happily be turned early to a chivalrous attitude toward all women when it is developed by suggestion and other training. In giving up a chair or bringing one for a guest, in lifting the hat, in noticing ways to be polite and attentive to mother, a lifelong conduct may be ensured.
Each day gives us trying and sometimes shocking revelations of the prevalent lack of courtesy, or even humanity, on the street cars during the "rush" hours. The indifference to the comfort of women, even the aged, on the part of many men and boys in the matter of giving them seats or other care, indicates a dangerous social condition.
The mother, instead of exercising selfish concern for her boy, should make it her duty very early to suggest that he give his seat to a woman or girl, as he would be glad to have someone do for his mother or sister. Such unselfish service will become a habit of pleasure, and help the boy become a pure-minded, manly gentleman with that respect for womanhood without which a nation is doomed.
There are a number of theories advocated by late authors on the "psychology of play," in which they connect the free and easy play of the modern child with the more serious and sober pursuits of our ancestors—our racial parents of prehistoric and primitive times. We quote from Worry and Nervousness:
And so we are told that the spectacle of the young infant suspending its weight while holding on to some object, and the early instincts so commonly shown to climb ladders, trees, or anything else available, are but racial mementos of our ancestral forest life. The hide and seek games, the desires to convert a blanket into a tent, the instinct for "shanties"—which all boys universally manifest—we are told that these forms of play are but the echo of remote ages when our ancestors sojourned in caves, lived in tents, or dwelt in the mountain fastness. In this same way the advocates of this theory seek to explain the strange and early drawings which the young lad has for wading, swimming, fishing, boating, and other forms of aquatic recreation.[5]
In this chapter we purpose to discuss the play of the child, whose career we will divide, for convenience, into three stages:
5 William S. Sadler, Worry and Nervousness, p. 377.
As nearly as is possible the little child should be out of doors the greater part of his waking hours: To our mind it is nothing 391short of criminal to keep the little folks in the house when the weather permits outdoor life.
Of the outdoor games which we have to suggest, perhaps the sand pile stands at the head of the list. Clean white sand should be placed in an inclosure just low enough for the child to climb over. Many, many happy hours may be spent in this sand pile, at the same time the little fellow is in his own yard and the watchful mother knows the drift of the conversations which take place.
In a previous chapter we called attention to the fact that the little girls' frocks should be provided with knickerbockers, so that she may run and jump, or sit as comfortable as the little boy, without a conscious reproof ever ringing in her ears, "Mary, do keep your dress down."
Tree climbing is another source of enjoyment to these little people and they should early be taught how to climb. Instead of suggesting fear to the child let the mother go into the yard and talk with her something like this: "Now, Mary, put your foot in that fork, now catch hold of that upper limb, hold on tight, you will get there yet;" instead of the following conversation, which all of our readers have heard: "John, do take care or you will fall and break your neck; be careful, you will fall. There, I knew you'd fall!" etc. Both mothers are trying to accomplish the same thing—one mother suggests "fore-thought," while the second mother thoughtlessly suggests "fear-thought."
These little people should be provided with rakes, spades, and hoes, and a portion of the yard should be given them in which they are at liberty to dig and rake and have a royal good time. We have yet to see the child who is not interested in flower-bed making, and the mother should think of the virgin opportunity to instill the story of life into the child's mind as he plants the seed, and day by day watches its development and growth.
A pen of rabbits may be a good thing, if proper measures are taken to prevent their burrowing out of the pen, destroying392 the lawn, causing much sadness of heart to their little keeper, and no end of annoyance to the neighbors.
Roller skating and hoop rolling, as well as sledding, are all valuable recreations. The snowman, snowballing, and the sled riding all bring the ruddy glow of health to the cheek, and are wonderful producers of good appetites and restorers of "tired out nerves."
There is no end to the number of things that can be done when the weather shuts us in, but before we take up these games let us never forget that every child thoroughly enjoys going out in the rain well protected with rubber boots, raincoat, and umbrella.
It is not extravagant to burn plenty of electricity or gas on cloudy days, for the artificial sunlight helps to cheer the heart. Such indoor games as those which may be had from blocks, puzzles, cutting out of pictures, darning of cardboard, soldier games, dolls, housekeeping, etc., are all splendid means of recreation for the little ones. Let the mother or caretaker join with the little folks in these pleasant games. For the older children, checkers and dominoes are most excellent indoor games.
First of all we must decide upon the bedtime hour, as well as the hour for rising. Between the ages of six to twelve, the bedtime hour should be eight o'clock, or not later than eight-thirty, and the rising hour at seven, or seven-thirty in the morning, for children of this age require eleven to twelve hours sleep.
Again, there must be taken into consideration the home work that the children at school are asked to do by their teachers. While this home work is not usually taxing, yet the time spent in doing the work must be taken account of. In our opinion the best time for home work is an hour and a half to two hours after the little fellow gets home from school. He should be allowed to relax for one and a half or two hours, to play out of doors whenever the weather permits, and then with either393 his mother or his caretaker from one-half to three-quarters of an hour should be spent on the lesson for the following day. Following this, the dinner hour is enjoyed with the parents, and after that there should always be provision in the daily duties of the father and mother for at least a half hour for the evening romp; so that play and recreation during the school age occupies possibly not more than two or two and one-half hours a day outside of school hours.
The playgrounds of schools are of inestimable value, and we quite agree with one who said: "If we can only afford one of the two—the playground or the school—have the playground first and afterward the school." The small parks and playgrounds of the cities are a great blessing to the little folks.
The companions of the school child are usually his playfellows at school, and we urge the throwing open of the home during inclement weather to allow these school friends to come in and make trains out of our chairs and tents out of our couch covers, steamer rugs, afghans, etc.
We do suggest that caution be used in allowing children to play indoors who are suffering from colds in the head, running noses, running ears, tuberculosis, or other chronic disorders, which are often highly contagious. Running noses and running ears, as well as tuberculosis, may be contracted by susceptible children when the play at recreation time takes place indoors; while such disorders are much less dangerous in connection with outdoor play.
We are well aware of the fact that some playmates may choose the bathroom, requesting that doors be locked, or wish to play in a bedroom securely away from mother and the caretaker. Under no circumstances should this be allowed. Let the child early learn that good wholesome play in the open is better than secretive misdemeanor behind closed doors.
It is a pitiful fact that many mothers apparently are wholly unconcerned as to the whereabouts of their little folks, even394 after dusk; this is unwise to say the least, for a boy or girl under twelve years of age should be found under the parental roof at dusk. The city mother should impress upon her child that when the street lamps are lighted his first duty is at once to come into the house. During the winter months this lighting of the street lamps occurs anywhere from four to six. During the summer months another rule should be laid down, depending upon the neighborhood, the character of the friends on the street, the surroundings, etc. By all means let us see that our young people are in the house by dusk.
Every mother who reads these lines has had to meet this question: "Shall I let my little one begin to go to parties?" and every mother will have to answer that question for herself. We personally feel that the social life extended by the school, together with the meeting of the companions at Sunday school, in the park, or on the playground, is quite enough; and we deplore the fact that many children grow into the idea that much time must be spent at "parties" in the drawing-room under unnatural surroundings, in dressed-up clothes, eating ice cream and cake, etc. Outdoor gatherings of children are wholesome and hygienic, but most of these indoor gatherings of groups of children we consider decidedly unhygienic. One child coming down with scarlet fever, measles, or whooping cough can infect twenty others at an afternoon party. The eating of so much ice cream, candy, and cake is deplorable in that it upsets the digestion, and all this is irritating to the developing nervous system of the child; and not infrequently brings on a lot of other symptoms, resulting in discomfort and disease. We believe in outdoor picnics but not in too frequent indoor parties.
Groups of children gathering in the park, on the beach, in the woods, when well chaperoned, are among the pleasant and profitable pleasures of childhood. It is just such gatherings that mothers and children should indulge in—and once a week395 is not too often during the long vacation. The mothers, too, should enter enthusiastically into the joys of a day's outing, where the enormous intake of oxygen, the hearty laughter, the races, the games, etc., all create a wonderful appetite, which can be so delightfully satiated from the well-filled lunch baskets; and while the children are thus playing together what a wonderful opportunity for the mothers to engage in an exchange of helpful ideas. Each mother has her own way, which is "the best way" to make this cake or that salad; or has met this particular difficulty in child training in a carefully thought out way; a neighborhood women's club can thus be held out in the open, while the children are having the time of their lives in the frolic of the picnic.
The movie is an institution that has come to stay, and today mothers everywhere are perhaps discussing this particular institution more than any other. The movie affords a wonderful opportunity to see the sights and scenes of other lands, of feeding the imagination of the child on travel pictures and nature pictures. It is a most deplorable fact, however, that this wonderful institution which is fraught with so many opportunities to educate and enlighten the mind of the growing child has carefully to be censored. Women's clubs have done much to purify the movies for the school-age child; many theaters are now showing on certain days a special afternoon movie for the children; and while many of these movies have great possibilities for good, we most earnestly urge that the school child see the movie that he is to see before dinner, and not have his mind excited and his nervous system "thrilled" just before going to bed. Someone asked me several years ago, "Are you going to let your little fellow go to movies?" I instantly answered, "No, but I shall take him." If the mother or the father sits by the side of a growing child and carefully, thoughtfully, and, yes, prayerfully, points out the good and explains the evil, then even the questionable movies will prove the means of bringing father and son and mother and daughter, into closer companionship.396
Under no circumstances should children under twelve years of age be taken to long lectures, entertainments, or concerts, which will keep them out until eleven.
Let the vacation be well planned. This is the opportunity "de luxe" for the child to earn a few pennies to enlarge his bank account. Allow him a truck garden, guinea pigs, chickens, anything remunerative, which will enable him to become one of the world's workers and one of the world's savers. Let him start a bank account when he is six, and watch him as he puts the dime in the bank, instead of taking it to the ice-cream-soda cashier.
Some time during the vacation, if possible, mother and father should accompany the little folks to the camp, to the beach—somewhere, anywhere—to get back to nature and live like Indians for a short time. Each member of the family will come back rested, happier, and more ready for the next year's work.
In the summer time learn to eat on the porch—it is great sport for the children. Many meals can be served on porches that are so often served in hot, stuffy rooms.
The "home" does not consist in the furniture, the rooms, the bric-a-brac, or the curtains. The home is the mother and the father and the children and the spirit of good fellowship which should possess them. Make the companions of the little folks very welcome, letting them learn the early use and abuse of the different articles of furniture in the house. It is all right to play tent with the beautiful couch cover; it is all right at certain times to dress up in father's best clothes and mother's beautiful gown, but while they are thus having a good time let them learn that all these things are to be used and not abused.
The homely boy or the homely girl usually grows up free from the flattery and undue attention which are sure to be heaped upon the good-looking boy and the popular girl. Way back in the early days of five or six, and all the way up to the ages of twelve to twenty, children should be taught that it is397 altogether natural and correct to do things well and to look well; parents should stop, and cause their acquaintances to stop, "making over" the boy or the girl just because they have done something well, or have beautiful curls, or because their eyes are a magnificent brown, etc. If a girl should be especially endowed with a charming complexion, a wonderful chin, and if she does possess a beautiful nose or neck, let her early realize that she has been made the custodian of goodly features and that she must give an account for this particular blessing, and under no circumstances must she become self-conscious about it. Ofttimes a good frown to an unwise friend is all that is necessary to stop this "lip service" flattery.
The "chewing-gum girl" is just a thoughtless girl, that is all; sit her in front of a mirror and compel her to chew gum for one-half hour and watch herself do it, and it will often suffice to cure her. Young ladies should be taught that chewing gum should be done in the bedroom, but never in the living-room or on the streets. It is not only a disgusting habit, but it often creates an occasion for criticism as to the quality of one's home training.
The mother who cares will not allow her lovely daughters nightly, or even semi-weekly, to frequent the ice-cream parlors and secluded soda fountains. She had far better arrange group dinners and group receptions in her own parlor; with ice cream served in her own dishes and eaten with spoons that she has supervised the washing of.
Young women and young men in their late teens crave companionship, and they should have it; but let it be under wise chaperonage at home or in public rooms, and not in the solitude of a lonely bench in the public park, or the seclusion of an out-of-the-way, ice-cream parlor. This "running the streets" which is so freely indulged in by the adolescent youth in the early teens need not occur, if wise provision is made for the assembly of small groups in the home.
Some elders think it pleasing and cute for young men and young women—fourteen to sixteen, or even seventeen—to398 wrestle and roll around on the floor like two huge kittens; but it is unwise and indiscreet and should be discouraged.
We hesitate to speak of dancing for we realize it is a very popular indoor recreation of today, but we most earnestly urge that if dancing must be done, it be done under proper chaperonage, and if young people must meet in public dance halls let them be municipal dance halls, where motherly matrons are in charge. Many of the social dances which bring the participants into such close physical contact are to be discouraged and stricken off the list; and while dancing is a splendid form of exercise—let us add that it is also sometimes a dangerous one.
After the boys and girls graduate from grammar school they may come into contact with such agencies as secret societies—which nine times out of ten are questionable—and while we realize that there is a contention both for and against these organizations, we may dismiss the subject here by simply adding that we have known little special good to come out of these societies.
While it may not be any more wrong to hit a ball from the end of a stick—as in billiards—than it is to hit it from a mallet in croquet; or from a stretched tendon, as in tennis; or from a bat, as in baseball—we do not feel that we have to argue the point, when we remind the reader that billiards and pool, especially in the public parlors, do assemble questionable companions, who use questionable language; while these games are often accompanied by betting, which is always to be deplored. And so with card playing, we see no greater harm in playing a game of euchre, than a game of authors, as far as the cards are concerned, but your boy and girl, as well as mine, as a rule, have cleaner and purer minds at the home game of authors than is probable in a game of cards in a public place.
In closing this chapter we have to announce a group of wholesome recreations which may be entered into by our lovely399 young people—the man and the woman of tomorrow—whom we one and all wish to keep clean and good and pure; all the while helping them to develop the sense of humor and the element of play. Such recreations are tennis, golf, croquet, roque, boating, sledding, skiing, bicycling, motoring, horseback riding, and a host of others too numerous to mention. Let us not forget that ofttimes pursuits such as garden-making and helping the parent in the office or in the home, may be made a great source of enjoyment to the adolescent youth, if they are allowed to earn a small amount of money each week, which they may deposit in the bank.
We close this chapter "Play and Recreation" with the wish that all, old and young, would develop a greater sense of humor, a greater love for play and recreation, which will increase the health of both mind and body and prevent many nervous disorders such as neurasthenia.
In every neighborhood there is to be found the delicate child, and everywhere anxious mothers are putting forth every effort to improve the condition of their puny boys and girls. In carefully looking over the puny child, we see an underweight little creature with pale skin, and as he comes to the table everybody notes that he refuses more or less food.
As we give the child a closer examination we find that certain lymph glands are enlarged, possibly adenoids are present in the post-nasal pharnyx, and, in many instances, there are badly diseased tonsils. Usually the puny child is constipated, hands and feet are cold, and he jumps and starts at any unusual noise, thus showing a tendency to nervousness. One of the first things necessary is to take this little one to a good specialist and if necessary have the adenoids and tonsils removed. This having been done, the diet should be carefully looked into. There should be served him for breakfast a generous bowl of dextrinized grains with a good portion of diluted cream, a glass of rich milk, a baked potato, and fruit. For lunch at twelve o'clock he should be given a glass of malted milk with egg, or eggnog, six or eight dates or three or four figs, a handful of pecan kernels, and perhaps a lettuce sandwich. For dinner at half past five, another nourishing meal of baked potatoes, a protein dish of either cheese and macaroni or eggs or meat, a generous fruit salad, a glass of rich milk, and bread and butter, should be enjoyed.
There is no class of little folks who eat between meals more often than do these delicate children, for mothers painstakingly401 endeavor to feed these children all they can possibly take; so one mother thoughtlessly went about it something like this: the half past seven breakfast having been only touched—nibbled at—with the ten o'clock hour came this request: "Mother, I am so hungry, I want something to eat." Eagerly the mother prepared either a meat sandwich or a jelly sandwich and possibly a glass of milk.
When it was time for the twelve o'clock dinner hour, or lunch hour, again the well-filled plate was refused, the appetite having been satisfied at ten o'clock. Having taken very little nourishment at noon, by half past two the plaintive plea again came to the mother ears: "May I have a piece?" and again the well-meaning mother gave him the desire of his heart. So the day passed, the dinner making the fifth time food was taken into the stomach, and in all probability there was eaten a cookie in between. The reader can readily see that the digestion was consequently very much disturbed, fermentation occurred, decomposition of food took place in the digestive tract, with its result—constipation.
Not a morsel should pass the lips of any child, and particularly our delicate child, between meals. Let him come to the table at half past seven or eight o'clock, and if he does not want to eat tell him frankly that that is all he is to receive until twelve—and stick to it. Nothing more than water or fruit juices should be taken between meals.
It may be necessary to create an appetite for the three meals we have just described, and as we now take up the outdoor hygiene we would not forget that some simple treatment should be instituted each day in a well-heated bathroom or bedroom. Roller skating or ice skating, hoop-rolling, rope-skipping, and Irish mail, or a coaster, all furnish splendid exercise for the delicate child. Under no circumstances should he be allowed to remain all the time in the house; and so pleasing recreations must be provided for him out of doors. The sand pile should not be forgotten, flower-bed making, raking the lawn, a polished coasting board fastened in a slanting position to an upright402 which can be mounted by means of a ladder, create splendid outdoor sports for these children.
Take the child into a warm bathroom each morning and let him stand in six inches of well-warmed water. With a rough mitten made out of either mohair, crash, or turkish towel, the entire body should now be rubbed until it is pink. This procedure is known as a dry-friction rub. Do not stop until the skin is pink, particularly the arms and legs, for the back and chest usually get pink quickly. Then with simply a cold dash of water to the feet, dry them well and allow him to dress. Twenty minutes before the meal hour, let him get out of the house and roller skate around the square as many times as he can in twenty minutes, or let him race and have a royal good time in the fresh morning air and then after this forced oxygen intake let him come in to breakfast.
And now for school, and as we say "school," we regret that there are not more "open-air schools." Some day the American people, more particularly the American mothers, will awaken to the fact that we need more schools with simply window space rather than so many closed glass windows. Some day we will send our children with sweaters, leggings, stockinet caps, mittens, even in the cool days of spring and fall, to "open-air schools," and in the cool fresh air they will think better and work faster and make wonderful progress in both studies and appetites.
The particularly delicate child, under treatment, will not spend the whole day in school. In all probability the forenoon session only will be attended, after which the half-past-twelve or one-o'clock meal that has been previously described will be given him. Now if the appetite is variable, arrange a little surprise for him by serving this meal on the porch or in the living-room by the open grate, or out under the trees. In all probability such a meal will be taken eagerly, particularly if the mother will read a pretty story. Now the afternoon is to be spent in doing a number of different things. We would like a pleasant walk, a visit to the park, hoop-rolling, roller403-skating, rope-skipping, ice-skating, outdoor sliding, anything that will take our little fellow out of doors to increase his oxygen intake until possibly the half-past-three hour is reached, when he should come into the house and lie down and prepare for the treatment for that particular day.
Twice a week he should be given a salt glow (described in the Appendix). Twice a week he should be given a thorough soap shampoo (also described in the Appendix). After each of these baths a special rub should be administered to the spine, and as there is so often spinal curvature in these children, certain stretching movements of the spine are valuable, together with hot fomentations (see Appendix) over the spinal centers. These are wonderful stimulants to the delicate child and should precede the salt glow twice a week. Every afternoon a hot-and-cold foot bath may be given to create a better circulation. The feet are put in hot water from three to five minutes (as hot as can be borne), and then they are quickly plunged into the coldest water obtainable for three seconds, then back into the hot water, and vice versa, until three changes have been made, always finishing the treatment with the cold dip. On the three remaining days of the week at half past three, the child will simply relax in the hammock or on the porch couch while the mother aids in the relaxation by a pleasant story. We would suggest that on Monday the salt glow be administered; Tuesday a rest is taken; Wednesday the soap shampoo is to be administered; Thursday another rest; Friday a salt glow; Saturday another rest, and Sunday the shampoo, etc.
Before going to bed at night, with the mother's hands well oiled with either olive or sweet oil, the circulation is again stimulated by the heavy friction rub.
Constipation is taken care of along the same lines as mentioned elsewhere in this book.
It is surprising to see how often these delicate children are infested by worms, and while a great deal of dependence cannot be put in that single symptom "grinding the teeth at night," or "pallor around the mouth," yet we do believe that many404 a delicate child continues to suffer from worms many years. It is a very simple procedure to obtain a specimen of the stools. A cathartic should be given and after usual free-bowel movement, the second time the child desires to go to stool this should be saved and taken to the laboratory for a careful search for worm eggs which are usually in evidence if worms infest the child. The treatment for worms is described elsewhere in this work.
We have seen scores of young people between the ages of eight and eleven who, before treatment, were pale, listless, under weight, irritable and cross, after three months of such treatment as has been outlined gain six to ten pounds and look as ruddy as their healthiest neighborhood friends. It is perfectly marvelous to notice how a child will put on from six to eight pounds in a short period, at the same time overcoming his irritableness and fretfulness. I am more and more inclined to believe that most bad children are sick children—are undernourished children—and it behooves us American mothers and fathers to give proper attention to this undernourished child, call a halt, and devote three months to giving him the help that he needs. He did not ask to come into this world; and it is "up to us" to give this child what he deserves—for every child in this world has a right to be well born, to be well fed, and to be well reared.
We confidently believe that most of the sex immorality seen in young people is more or less the result of ignorance and curiosity; therefore we most earnestly desire in this chapter to portray so interestingly the beautiful story of life as seen in the vegetable and animal world, that our mother-readers will be seized with the great desire wisely to convey to the young child's mind this sublime and beautiful story. The questions most naturally arising in the mind of the reader at this time are: When shall we begin to tell this story? How shall we tell it? Where shall we begin? Where shall we stop? Realizing full well that the subject is usually handled prematurely and with unpreparedness, we will attempt in this chapter to discuss it with courage and candor, believing that there is a right way, a right time, and a right place to impart this information.
When the little folks are about three or four years of age, when confidence and trust are at their height, they often come to us begging for a "story;" and this is the golden opportunity for the parent or caretaker to tell them the story of Mr. and Mrs. Corn, and all their little babies; or Mr. and Mrs. Morning Glory and their little folks. There are a score of other equally interesting and instructive botanical stories which are just as beautiful in their sublimity, and fairy-like in their personality. The little children's eyes grow big with wonder as you tell the story of a whole township of families by the name of Corn (See Fig. 17), who have their residences out in the wide country fields.406
We will first introduce the child to Mr. Corn, the tassel, waving proudly and majestically in the breezes, and seeming to say: "I am master of all I survey." The little fellow is filled with wonderment as he learns how the clouds give up their drops of water to quench his thirst and how the sun smiles upon him to yellow his beard; and how the wonderful all-important pollen is developed and ripened.
Often the child eagerly asks, "And where, mamma, is Mrs. Corn?" and to that interested upturned face we relate the pleasing story of the beautiful silken tresses of Mother Corn. Early in her life she is a beautiful shade of green, and as she thus gracefully hangs out from the ear of corn, day by day the smiles of sunshine turn this mother corn to brown, and then to a still darker shade.
"And where, mamma, are the babies?" the child next inquires; and, as we take the ear of corn, removing the outer clothing—the husks—we find the underclothing, a much lighter shade of green, and here now we are in close contact with the babies themselves—the kernels—and to each little kernel or baby corn we find mamma closely clinging. Here is a beautiful opportunity to teach mother-love and mother watchfulness, as also the opportunity to draw lessons from the baby kernels sitting there in even rows, with their faces clean, silently contented—just doing their duty. The stories that may be told are limitless, and possibly as interesting as are the myths and fairy-tales, yet all the while as true as truth itself, with no fakery, no legends—just simple truth.
Now on a second trip into the cornfield, another story may be told of the important work of the pollen. This "father part" of the plant falls upon the silken tresses of the "mother part," by which the pollen is carried down to the sleeping corn-baby seeds—the kernels. And when the "corn dust" does reach the sleeping seeds a great change begins to take place. This change is known to the adult as "impregnation;" to the little child it may be presented as "an awakening" of the sleeping seeds, so that they begin to grow, to develop, to expand and408 push out, until we have the full-grown seeds seen in the delicious and juicy roasting ear.
Sometimes, in the case of the larger plants and trees, Father Tree may be miles and miles away from Mother Tree and so this all important pollen must be carried by the wind or by the bees, and as it blows against the mother part of the plant-flower she catches it and pushes it downward to the seed babies. The wind scatters the pollen of the oak tree, the hazlenut, the walnut, the birch, the willow and many others; for, without the good kind wind or the bees, the pollen would never find its way to many a mother flower, and the "fertilization" of the seed could not take place.
Perhaps the story of life can be told as beautifully from the morning-glory as from any other flower. Here the beautiful flower cup is the home of Father and Mother Morning-Glory and all their little babies. (See Fig. 18).
As we carefully take away their little home, the flower cup, we have left a little green cup, and coming up from the center you will see five little stems, every one of them wearing a hat of powder or pollen and this—if you please—is Papa Morning-Glory. Look closely and you will see coming up from the center of these five stems (stamens) one central stalk without a hat, Mother Morning-Glory, known in botany as the "pistil"; and as you follow down this pistil you will find an enlarged part at the base, which is known as the cradle-nest—the home of the seed babies.
Little was known about this wonderful fertilization of the seeds by the pollen two hundred years ago, and a whole century passed before the secret of the blossom and the bees was discovered; and even then it was not fully realized how great was the work of the bees in cross-fertilization. Nor was it understood that the beautiful blossom of the flower, with its sweet nectar, was an exceedingly important factor in attracting the bees. Another century passed before Darwin gave to the world the story of the great work performed by the bees in cross-fertilization—in carrying the pollen from flower to409 flower, for it is now a well-known fact that all of the blossoms visited by the bees produce better fruit and better flowers.
In the flower where the father and mother part matures at the same time, self-fertilization is the rule. Cross-fertilization occurs in instances where either the father part or mother part ripen at different times, in these cases the pollen is carried from plant to plant by the wind or by the nectar-seeking bees. These busy bees, with their fluffy little feet and fuzzy coats, become completely covered with this all-important flower dust, and in seeking nectar from other flowers they leave the "awakening dust" behind, and thus cross-fertilization takes place; new types of babies are produced, new generations of fruits and flowers.
Dr. Chadwick, in her Blossom Babies, gives us a beautiful recital concerning the fertilization of plants, which provides an endless number of interesting stories. The water plants are very interesting in that the pollen is just light enough to float on the exact level of the mother part of the flower, otherwise fertilization could never take place, and there would be no more lovely lilies. Long throated blossoms are fertilized by their attraction for certain moths or humming birds who have long tongues. Mother Nature is exceedingly careful to reproduce her children, and in every conceivable way she sees to it that her plant-seeds are fertilized and distributed. We are all familiar with the dandelion and the thistle and a host of others which fly through the air with actual plumes, some seeds fly with wings, such as the maple; other seeds travel by clinging or sticking, such as the cockle burr; still others float and shoot; while we all know about a lot of seeds that are good to eat, such as the nuts and fruits, as well as many of the grains, such as corn, etc.
An incubator about hatching time is a wonderful object lesson in teaching the story of life. Take the children to visit one and let them actually see the live baby chicks coming forth from the seed-shells. Other wonderful lessons may be drawn from the mother horse or the mother cow; and it is impossi410ble to portray the close companionship, the sublime trust and confidence, which exists between the mother and the child who have been bound together by these ties and sentiments of truthfulness, trustfulness, and frankness.
The little fellow is daily learning that everything that grows comes from a seed, even the salmon which was eaten at lunch yesterday was the text for an impressive story about Papa and Mamma Salmon. In the beautiful Columbia river Mother Salmon is swimming about quietly seeking a shallow place in the stream where she may deposit her cluster of baby seeds, which looks very much like a mass of tapioca pudding as they gently sink to the bed of a shallow spot in the river. There they lay "sound asleep" until Father Salmon, swimming by, is attracted to the spot and, hesitating, talks something like this to himself: "Why the idea, here are some helpless fish-baby seeds, they can't grow and develop without me, here they are sound asleep;" and, nestling over them, he contributes the self-same and all important "something"—comparable to the pollen of the plants—which wakes them up. In the case of the fish the "awakening" substance is not in the form of a powder as in the plant world; but is in the form of a semi-liquid mass, much resembling the white of an egg. The little seeds soon begin to tremble—begin to wake up—and then begin to swell and grow and develop. In a few days what do you suppose happens to these little bulging baby seeds? The very same thing that happened to the chick seed—they burst and out come hundreds of cute little fish minnows. In just a few hours they are all swimming about in a most wonderful fish-like manner.
Some day you will be surprised by your little child suddenly asking you some such question as this: "Mother, where did I come from?" while in the same frank manner you reply: "Why from your mamma, of course; where do you think you could have come from? Everything that grows comes from411 its mamma—oranges, apples, radishes, cabbages, cats, dogs, and chickies—everything that grows has to have a mamma and papa," and they are often satisfied with this answer for a long time. No child should go to kindergarten without knowing that he came from his mother, and this knowledge should come to him from his own mother's lips. These are different days than those in which our grandmothers lived. The spirit of investigation and of inquiry is in the air. The moving-picture show makes it necessary for children of nine or ten to understand these things—to have a knowledge of certain of the conventionalities of life. Twenty years ago this may not have been so necessary—the youth of that day might have waited several years longer for certain phases of his sex instruction. It is highly important that this knowledge be obtained from a wise and pure and sympathetic mind—from the child's own parents.
One mother put her little girl's questions off week after week, saying: "I will tell you when you get older, dear—no, not now, dear; run away, you are not old enough to know such things, you must forget about them." Thus the unprepared mother sought to gain time in which to consult the doctor or the library. Finally the day came when the mother felt that she was sufficiently wise to answer the query, "Where did I come from," and so with her heart in her throat she approached her daughter, saying: "Come, Mary, mother is going to tell you all about it. I am now ready to answer your question." Imagine her surprise and astonishment when Mary said: "Oh, you needn't mind, mother, Kate told me all about it last week." Now the question in my mind is: how did Kate tell her? How much unnecessary information did this older and experienced Kate put into the pure mind of this innocent little girl?
One mother in a western state—a county superintendent of schools—told us the following interesting story of her own experience, which we think may be of help to some of our mother readers.412
One morning her seven-year old son rushed into the house exclaiming: "Oh, mother, there is a new calf out in the barn, and I know where it came from; I saw a wagon load of calves come by here yesterday, and one of them must have dropped off, for it is right out there in the barn with old Bess this minute."
The mother was very busy with her papers and her reports, and she let the incident pass with a smile, thinking it was a very pretty little story. A week later the six-year old brother came in saying: "Mother, I think there must have been another wagon load of calves passed by, and one must have been lost off, for old Nell is cleaning up a little calf out in the barn for all she is worth," while the older brother piped up: "Sure, it was another load of calves; that is just exactly the way the other calf got here;" and the two little fellows went off to school.
About a month later that county superintendent suddenly became a much wiser mother than she was before, although her heart was made to ache. Both boys came home from school one day and the older one met her with something like this: "I am mad! I've been lied to; all the fellows at school say I have, and they are making sport of me, too," and with a glare in his reddened eye he continued, "You know that new calf did not come off that wagon; you know that calf came from old Bess herself; all the fellows say so at school, and they are making all kinds of fun of me, and I don't want to go back. I'd like to run away from home." The mother quietly drew the boy to her side and reminded him that she had simply listened; that she had not opened her mouth; that he came into the room and told about the incident himself, but this did not satisfy him. He turned to her wounded and crushed, saying: "Well, you let a fellow believe it, and that's just as bad;" and this educated mother—this trusted custodian of a county full of school children—beseeched me to warn mothers everywhere to teach their children the truth, and to never let a child go to school with a sex misunderstanding. She told me that it took her six months to get that boy's confidence back again.413
I believe that many mothers make the sad mistake of showing the child that they are shocked by trivial sayings and trifling experiences of their little people. If we could only get it into our heads for once and for all that our children are born into this world veritable little thieves and falsifiers, as well as adventurers and explorers, we would then cease being so shocked and outraged by their frank statements of what they have heard or have done. Let the mother listen to all these things with calmness, while she seeks to direct the child's mind in pure and elevated channels—to help him upward by imparting "precept upon precept; here a little and there a little."
Children will come in with stories that at first thought do greatly shock the parent; but under no circumstances should the boy or girl discover that the parent is shocked, for if he does he will not likely come again with another such "shocking" difficulty. One mother told me that her seven-year-old boy, beginning third grade, came into her bedroom one morning saying: "Mother, I am just busting to say something," and this mother very wisely said, "Well, say it; certainly I don't want you to burst," and she told me that this boy whispered to her three of the filthiest words that he could possibly have heard on the streets. In relating this experience to me she said: "Do you know, doctor, that I really did not know what to think at first, but I remembered that you had taught me never to be shocked, and so I looked up and asked: "Do you feel better?" whereupon he breathed a big sigh and exclaimed: "What a relief! I have just been busting to say that to somebody." Mother, to whom would you rather he would say these things? to you, or to some little girl out on the street, or to some older boy? Think what trouble and possible mischief were avoided by whispering into the sympathetic ear of mother. This wise mother turned to that little boy and said: "Son, that ear is always waiting for just such things and whenever you feel like saying something—like getting it off your mind—you just come to me;" and he came repeatedly. One time he came in saying: "I don't know whether you want me to play with Harold or not; he does414 some of those things you told me about the other day." And the mother thoughtfully and wisely looked up and said: "Did he do it in front of his mother? Why of course he didn't. Did he ask you to go into the bedroom or bathroom and lock the door?" and the little fellow quickly answered: "Why sure he did; how did you guess it?" and added "now I suppose you are not going to let me play with him any more," and this wise mother, knowing that if she denied him this privilege that it would quite likely be frequently sought, said: "Why, certainly play with Harold in the open, but whenever he suggests secrecy—" she did not have time to finish the sentence, the boy said: "I am wise; whenever he gets to doing that 'funny business' I'll skiddoo." The confidence between that mother and son, to my mind, was wonderfully sublime—all the while practical and helpful in his daily training.
A little older child sees the fowls, the dogs, or the cats, "mating," and then, rushing into the house, inquires what it is all about; and unless the mother is on her guard some older member of the family may show surprise and thus thoughtlessly convey to the child's mind that his question is improper and entirely out of place. To the question, "What are they doing, mamma?" quietly answer, "Just mating, dear, just as the flowers mate; everything that lives or grows comes as the result of mating."
Suppose that you were repulsed every time you approached a dear friend, your husband, or some other member of the family? Take, for instance, the matter of a caress or an embrace—how would you react to repeated rebuff? And so with the little child; he comes into this world full of confidence and trust, full of wonder and curiosity; possessed with the spirit of exploration and investigation—everywhere and all the time he asks questions. Usually, his questions are answered thoughtfully and without hesitancy, except along the line of one thought—that of sex. Do not think for one moment that he is satisfied by your evasive answers. You have but to recall your own childhood experiences, and415 remember that today the moving picture show and general public sentiment has placed the age for such knowledge from one to five years earlier in this generation than in the past. I do not care what the child comes into your presence with, be it the most shocking thing in this world, do not under any circumstances let it disturb your mental poise, or raise your ire or shock you; for if you do, then and there—at that moment—occurs a break in the sublime confidence which the child reposes in you.
While we are using the plant and animal world as object lessons in teaching our children the facts of sex and the secrets of life; while we face the commonplace sex matings of the animals about us without cringing, without appearing to be shocked when our children call attention to these things; nevertheless, when the child is old enough to take cognizance of these phenomena, he is old enough to begin to receive some definite instruction from his parents regarding the moral phase of these great biologic problems. We cannot safely and indefinitely utilize the animal world as an object lesson in sex education, without at the same time emphasizing the moral difference between man and the beast.
Many parents treat these sex problems so lightly and endeavor to act so naturally and unconcerned about these questions, that the child comes to look upon the promiscuous sexual relations of the animal world as something altogether natural; and, unless proper moral and religious training is carried on at this time, he stands in danger of coming to regard lightly the moral standards of modern society.
At the same time of life that Mother Nature fully develops the sex instincts—at adolescence—she also awakens the religious emotions; the one being so necessary for the proper and adequate control of the other. Let parents take a cue from old Mother Nature, and at the same time the sex relations of animals are freely discussed with the growing child, let the mother or father wisely call attention to the fact that but very few of the animals live family lives as do human beings. In this416 connection valuable use—by way of illustration—can be made of the ostrich and some of the ape family who are loyal and true to their chosen companions.
Moral and religious instruction must accompany sex-hygiene teaching just as soon as you leave the realms of botany and enter the sphere of zoology. We could here relate many a tragic experience which our patients have passed through as a result of volunteering too much sex knowledge and at the same time neglecting this very necessary moral instruction.
We must bear in mind that the child believes what we tell him; he trusts us implicitly and we owe it to him to teach him the truth in answer to his numerous questions. We must keep his confidence. Take the matter of Christmas, for instance. How many confidences have been broken over the falsehood of Santa Claus and the chimney. Two little fellows hesitated in their play in the back yard, and the following conversation was heard: "You know that story about Santa Claus is all a fake." "Sure it is, I know it isn't so, I saw my father and mother filling the stockings. You know that stork story is all a lie too, there's nothing to it, babies don't come that way, and now I'm investigating this Jesus Christ story, I suppose that's all a fake too." The fact of the matter is, that while these children have discovered the truth of the first two stories, for a long time they will query the third story, for to them, that too is mysterious and fairy-like. They hadn't seen Santa or the Stork and had only heard about Jesus.
The story of the human baby may be told to any child of seven to ten years. Each mother will have to decide in her own mind the right time to go into the details of the human baby seed. The child should have had an opportunity to have planted some seeds in the ground, to have visited an incubator, or to have visited the farm and observed the family groups of babies—the chicks, pigs, calves, etc.—with their mothers.
Let me see now how many different baby seeds do we know?417 Yes, we do know the radish seeds, many flower seeds, chicken seeds, bird seeds, corn, potatoes, and many others, and we can tell them all apart. The boy and girl baby seeds are too tiny to be seen with the eye. They are so small that it takes about two hundred of them in a row to make one inch. We can only see these human baby seeds with the aid of a microscope. It is such a precious seed that it cannot be intrusted to the ground or to a tree nest for development. The great Wise Father decided that a mamma would love and care for it better than anything or anybody in all the world. So, just as there is a cradle bed in the mamma flower, so there is in the human mother's own warm body, tucked far away from the cold rains and the hot sun, a little bed, for the boy and girl baby seeds. Right near to this little seed bed Mother Nature has prepared a little room, which holds the tiny "waked up" seed for nearly a year as it slowly grows into a little baby girl or baby boy.
You remember the story of how Bob Robin found Jenny Robin, don't you? You remember mamma told you how Bob came up from the southland early in the spring and asked Jenny in lovely bird song to come and be his very own wife? How he promised her he would feed her on cherries, and currants and the fattest of worms? And that she told Bob she loved him and went to live with him, and how they built that cute little nest to hold the eggs; and how Jenny Robin sat on the nest until the little baby robins were all hatched out.
Well, one day papa found mamma. He met her and loved her dearly and told her he wanted her to come and live with him, and they built their home nest and were very happy together, because they decided they would always love each other more than any one else in the world. After mamma and papa built their home and lived together, one day a wonderful change came to one of the baby seeds and it awakened and began to grow. Mother Nature whispered to it, and told it how to find its way into this little room and there it clung to the wall and grew for nearly a year. Papa brought mamma418 nice things to eat, just as Bob Robin did Jenny. Papa did everything he could to make mamma happy and comfortable.
For nearly five months this little seed just grew and did not let anybody know it was there, until one day it began to tap against the sides of the walls of this little room, and every time it did mamma's heart just bounded with joy as she thought of the precious seed growing to be a darling baby—and all inside of her very own body. And one day, after nearly a whole year had passed, the door to the room began to open, and, very soon, a lovely baby found its way out of this special room into the big, big world. Mother Nature then told this little baby that it might still remain close to the mamma it had been with so long, and so she taught it how to get its food every day from mamma's breast. At this point the child usually breaks out by saying, "Now, mamma, I know just why I love you so much."
I shall always remember with pleasure my own son, not quite two-and-a-half years old, who sat at the table one day asking numerous questions such as, "Mamma, what is that? Mamma, where did that come from?" etc.
He picked up a navel orange, and pointing to the navel said, "What is that?"
I frankly said to him, "Why, my dear, that is the baby orange."
"Why, Mamma," he exclaimed, "do oranges come from oranges?"
"Certainly, dear child; where else could they come from?"
"But," he says, "Mamma, do potatoes come from potatoes?"
"Why, honey," I said, "Orange babies come from orange mammas, potato babies from potato mammas, grapes come from grape mammas, little kitties from kitty mammas, and little boys from their mammas."
We simply mixed all the babies up, just as you would mix up a delicious fruit salad. We took from the mind all question of mystery and surprise by quickly and honestly answering his question. Thus, his first knowledge of his origin, if he is419 able to recall it, will ever be associated with oranges, grapes, potatoes, kittens, etc.
We did not tell the whole story for some two or three years later, but day by day we simply answered the questions as he asked them.
One day, when he was about three, he burst into my bedroom, saying, "Mamma, dear, I did come from you, didn't I?"
"Why, yes, darling, from nobody else; just from your own mamma and papa."
"Say, mamma, was my hand in your hand, my foot in your foot, my head in your head?"
"No, dear," I replied, "You were all curled up as snug as a little kitty is when it's asleep, and you slept for nearly a year in a little room underneath mamma's heart."
It was a wonderful story. He threw his chubby arms about my neck, his legs around my waist, and said: "You dear, dear, mamma. I do love you and papa more, just awful much."
In my private sitting-room, where William and I have had many conferences, there hangs my medical-class picture with classmates and faculty. A member of my family was one day answering the boy's queries as to who this one or that one was, etc. Finally, on pointing to one particular face, the answer came to his inquiry, "That's Dr. P. You wouldn't be here if it wasn't for him." That evening the little fellow, just past three years, came to me and asked, "Mamma, didn't you say I came from you?"
"Yes, dear," I replied.
"Well, Auntie says I wouldn't be here if it wasn't for Dr. P. What did the doctor have to do with it?"
"Why, simply this, dear. The door to the little room in which you grew in mamma's body wouldn't open, and so kind Dr. P. came and helped open the door."
"And let me out?" exclaimed the eager child. "Oh, I want to go and see Dr. P. and thank him for helping me out!"
And this little fellow was neither shocked or surprised, any420 more than he was over finding out that orange babies came from orange mammas.
In the same frank manner in which the simpler questions are answered, strive to answer these important ones. If we seek to evade, to postpone, to wrap in mystery these sex questions, the little ones will not forget but will ponder and worry over them, and seek to obtain certain knowledge from others who oftentimes tell too much or too little, and such information is usually mixed with much unnecessary matter which may or may not be foreign to this particular subject. On the other hand, if we frankly and honestly answer the question at hand, curiosity is avoided and the child feels he understands it all. The subject drops into the background of his mind—into the marginal consciousness—with the countless other facts he has accumulated. A sense of "knowledge possession" is as comfortable to the child as it is to the adult.
Often the question arises: "Will they tell to other children this newly found knowledge?" If the wise mother makes them feel they are a part of a "family," and reminds them that such matters as the secrets about Santa Claus, the stork, and the baby nest are only discussed in "family groups," they are often seized with the normal pride which accompanies confidence, and often keep secrets as well or even better than do most adults.
One day a little man, three-and-a-half years old, was posing for a photograph. The photographer said: "My little fellow, you pose well. We've had such a good time together. Where did they get such a lad as you?"
The mother's heart stood still. From her hiding place behind a large curtain at the back of the studio, she listened, wondering what would be his answer.
At first he hesitated, but after a moment's pause, said: "Really, Mr. W. if you don't know I feel sorry for you, and I'd really like to tell you, but I can't, it's a secret between me and my mamma."
Children enjoy secrets. If possible, isolate a group of sub421jects that are not to be discussed with playmates, such as Santa Claus facts, the stork story, and the baby story; often the very isolation of one single fact stands out so big in the child's mind that he is many times tempted to mention it, when, if it were associated with a whole group of "family secrets" he would seldom be led to talk about it. As we have said, children can keep secrets much better than most adults; and just suppose they should tell something—what harm? With twenty-five false stories in the neighborhood, suppose one story of truth should escape! No particular harm would result; but I find they keep these secrets well.
Numerous questions will arise which should be met with open frankness. No blush, no shame, should even suggest itself, for we are dealing with a wonderful truth, so let us give out our answers with clean hearts and pure minds. The Great Father will bless us and surround our loved "flock" with a garment of confidence in mother and father that will protect from much of the evil which is in the world, and, eventually, our little ones will grow into men and women whose very life of purity will cast its influence into the social circle. Only the company of the good and the true and the pure will be sought when associating with the opposite sex; while, in the end, better mothers and better fathers will be developed for the work of the next generation.
1. The attention of the little folks is often drawn to the sexual organs by a sensation of itching which accompanies a state of uncleanliness and filth. The genitals must be kept scrupulously clean. Elsewhere in this book we paid our respects to the rubber diaper, and we wish to reiterate at this time that it is in all probability responsible for a great deal of masturbation. The constant moisture and heat keeps the genital organs in a state of congestion which is more or less accompanied by itching sensations.
2. A long or tight foreskin in the male child favors the accumulation of secretions which not only occasion itching sensations but oftentimes are the cause of convulsions in early422 infancy. In the case of the female, a tight foreskin over the clitoris will retain secretions which also cause an itching sensation.
3. Unscrupulous nurses sometimes actually teach these little fellows to masturbate.
4. Lying in bed on the back with a full bladder, in the case of the boy, often produces an erection of the penis, and this is usually accompanied by a feeling of fullness which serves to direct the mind to the genital organs.
5. Lying in bed alone with nothing to do but to investigate often results in secret vice.
6. The unwise practice of allowing children to visit each other over night and sleep together, is often productive of mischief.
7. Constantly telling a little girl to keep her feet down, to keep her dress down, makes her over conscious of sex and otherwise causes the attention to be directed in unhealthy channels.
8. Teasing a child unnecessarily about a little sweetheart often produces an emotional reaction which is not altogether desirable. These suggestions are especially bad in the older children.
9. Unwise sex knowledge is usually productive of curious investigations, which if not properly followed up, particularly in those children who are temperamentally secretive, and who do not fully confide in mother and father, often results in moral misdemeanors.
10. Do not allow two young children habitually to isolate themselves in their play. Direct their play away from the attic, the basement, and other places remote from direct observation.
There is no use telling a child not to touch that part of his body, particularly if it is a boy, for it is going to be absolutely impossible for him to carry out such instructions. One mother overheard her caretaker say, "Don't put your hand there, it isn't nice." Immediately the wise mother called the caretaker to her and reminded her that most children usually continue to investigate even though they are told not to, and so the care423taker received this instruction: "When you see Harry putting his hand to that particular part of his body, just gently draw it away and divert his attention to something else, and when he goes to sleep in his little bed teach him to lie on his side and bring his little hands up under his chin or the side of his face and remain near him telling him a beautiful story until the eyes begin to get sleepy and pick him up immediately on awaking in the morning."
This mother was quite unlike the mother who once came to my office, saying: "Doctor Lena, I have done everything to prevent my boy's handling himself, why every time he wakes up at night I am always awake and I instantly say to him, Charlie where are your hands? You see Doctor, I am doing the best I know how." Very likely it is unnecessary to call the attention of the reader to the fact that this mother was doing more harm than good in constantly calling his attention to the fact that he did have a sexual side to his nature.
And just here let us add that while masturbation is an unclean habit, an impure habit, and a thing altogether to be shunned, we would not be honest to ourselves and to our readers if we did not explain that under no circumstances does it make foolish minds out of sound minds or insane minds out of sane minds. If your boy or your girl is going to grow up to be foolish or insane he had a through ticket for the feebleminded institution or the insane asylum when he was born into the world. The time when masturbation does affect the mind of the child is when the mind awakens to the fact that it is allowing an abnormal, unclean, or filthy habit to dominate mind, soul, and body, and then, and usually not until then, does this bad habit begin to cause mental depression and a host of other symptoms that so often accompany masturbation.
In our worthy efforts to combat the evils of secret vice let us not go to the other extreme and create such a condition of mind in the youth of our generation as to lay the foundation for sexual neurasthenia later on in life, as a result of424 the protracted worry, constant brooding, and conscientious condemnation, which they so often experience following some brief or trivial indulgence in early secret vice. Let us fight this vice with the truth, and not resort to over-exaggerated pictures which can only serve to blight the hopes and destroy the courage of over-sensitive boys and girls after they have grown up—as they look back on their lives and recall perhaps a single misstep in their childhood. In this way we can hope to do good today without mortgaging the child's happiness and mental peace in years to come.
1. The Sponge Bath. The child, completely undressed but loosely wrapped in a wool blanket, is placed on a table so that the mother or a nurse may conveniently stand while administering the bath. Close at hand have a number of soft linen towels and a large bowl of tepid water which may or may not contain a small amount of alcohol, witch-hazel, salt, or vinegar, according to the doctor's directions. The upper portion of the body is partially uncovered and the tepid water is applied with the hands to the skin surface of one arm. The hands may be dipped in water from one to four times, thus making repeated applications of the water to the arm. These are followed by careful drying—patting rather than rubbing. The other arm is now taken, then the chest, then the back and last the legs.
2. The Wet-Sheet Pack. Two light-weight wool blankets are folded to fit the child; they should extend eighteen inches below the feet and should be wide enough to lap well in front. A sheet just large enough to envelop the body is then wrung out of cold water and spread out over the woolen blankets. The feverish child is entirely disrobed and is placed on the wet sheet, which is quickly wrapped about the body, over the chest, under the arms, and between the legs—coming in contact with the entire skin surface. The dry blankets are quickly brought around and tucked snugly about the patient. This is a cooling wet-sheet pack and will often so relieve the nervousness and irritability of a feverish child that he will go to sleep in the pack. In the very young child, under two years, it is important to put some accessory warmth to the feet such as a warm-water bottle—not hot. The effect of this pack is very quieting, and is indicated when the temperature of the child reaches 103 F. or more.428
3. The Graduated Bath. This is usually administered in a large bathtub and is beneficial in the fevers of the older children. The temperature of the water should be one or two degrees higher than the body temperature, for example—if the child's temperature is 103 F. then the bath starts out with a temperature of 104 or 105 F. The temperature is then gradually lowered, about a degree every two minutes, until it reaches 92 or 90 F. A helper should support the head while the mother or nurse briskly rubs the entire skin surface of the body. This friction greatly facilitates the fever-reducing work of the bath because it brings the blood to the surface where it is more readily cooled by the bath. This bath should last ten or fifteen minutes.
4. The Hot Sponge Bath. Often, in combating the high fever of typhoid, the hot sponge bath is valuable. The hands are dipped in water just as hot as can be borne and are applied to the chilly, mottled skin which is so often seen in high fever. This bath is administered just as is the tepid sponge bath. Evaporation is allowed to take place to some extent by delaying the drying. In this instance the child should be wrapped in a warm wool blanket with only a portion of the body exposed at one time.
5. The Hot-Blanket Pack. The hot-blanket pack is indicated at the onset of many fevers such as in typhoid, grippe, pneumonia, etc. Like the wet-sheet pack, the blankets are spread upon the bed, abundant accessory heat is applied—such as a half-dozen hot-water bottles. In the absence of these, glass jars or hot ears of corn may be utilized. Hot bricks or hot stove lids wrapped in paper are also serviceable. A blanket, in size to suit the individual (an adult would use a full single blanket, a child one-half of a single blanket), is wrung very dry from boiling water. This may be done by the means of a wash wringer, or two persons grasping the blanket by its gathered ends may so twist it that it looks very much like an old-fashioned twisted doughnut. The twist is now lowered into boiling water, and as each pulls the twist wrings itself. This is at once quickly spread out so as to let the child lay on the center, and then the hot sides are brought in contact with the429 skin, just as in the wet-sheet pack. The dry blankets are now brought quickly and snugly about the child. Just outside the second dry blanket the accessory heat is placed to the sides of the trunk, the sides of the thighs, and one at the feet. A wrapped stove lid or a hot-water bottle is placed over the pelvis and one under the back. Cold cloths are put on the face and around the neck, and these should be changed every three minutes. This pack continues for fifteen or twenty minutes, at the end of which time the accessory heat and the wet blanket are removed and the patient is cooled off by a cold mitten friction, a saline rub, a witch-hazel rub, or an alcohol rub; or the patient may be placed in a tub of water, temperature 98 F., after which he should be carefully dried off.
6. Sweating Baths. Another bath which is effectual at the onset of grippe or pneumonia is the sweating bath. The bowels should have moved some time before the treatment. Have ready a large bowl of ice water, two turkish towels, one sheet, and four wool blankets. The bathtub is now filled with water at the temperature of 100 F.; which is quickly raised up to 103 or 104 F. Ice-water towels are applied to the head, neck and heart. The patient remains in this bath for about ten minutes, after which he steps out and at once gets into the four hot, dry blankets previously spread out on the bed. No time is lost, the patient is quickly wrapped in the hot blankets and sweating continues for twenty minutes. The covering is now loosened and gradual cooling takes place. It is well to go to bed at once.
1. The Cold Mitten Friction. The cold mitten friction is a bath that is applicable to any condition where the child or adult needs "toning up." It should always be preceded by heat to the feet. The following articles are necessary. Four or five turkish towels, a warm wool blanket, a hot-water bottle for the feet, a bowl containing water, a generous piece of ice, and a rough mitten without a thumb. The patient's clothes are removed and he is wrapped in the warm blanket with heat to the feet. One part of the body is taken at a time, first the arm, then the other arm, then the chest, the abdomen, one leg, the second430 leg, and last the back and the buttocks. A dry turkish towel is placed under the part to be treated, and after the mittened hand is dipped in ice-water, brisk short friction strokes are given to the arm until it is pink. Several dippings of the mitten in ice-water are necessary. One cannot be too active in administering this bath. Slow, Delsarte movements are entirely out of place at this time. Action—and quick action—is a necessity. No part of the child's body is left until it is pink. It is an invigorating tonic bath and is indicated in all conditions of low vitality, functional inactivity, puniness, rickets, etc.
2. The Salt Glow. Fill the bathtub half full of warm water, temperature 100 F. Slightly moisten one quart of coarse salt. Stand the patient in the water, placing one foot on the side of the tub while you rub the entire leg with the salt until it is very pink. The other leg is treated in the same manner, as also are the arms, abdomen, chest, and last, the back. By this time he will be all aglow from head to foot. Rinse off the salt, and give him a cold dash with the hands or a spray.
Fill the tub with water at just 97 F., and remain in the bath for twenty minutes or more, with the eyes covered, all the while maintaining the temperature at 97 F. Dry gently with a sheet to avoid exertion and exposure. Go at once to bed.
Hot fomentations often relieve suffering and are indicated in such conditions as menstrual pain, abdominal cramps, colic, backaches, etc. A good substitute for fomentations may be given as follows: Fill a hot bag half-full of boiling water. Over this place a wet flannel and two layers of dry flannel. Apply for fifteen or twenty minutes over the skin area to be treated, finishing up with a cold water or alcohol rub.
A very effectual way of applying moist heat to any portion of the body is by the means of hot fomentations which are given as follows:
One-fourth of a single woolen blanket (part cotton) is folded and grasped at the ends and twisted like an old-fashioned dough431nut. The twist is then immersed in boiling water, the hands still grasping the dry ends, and then by simply pulling out the twist (widely separating the hands) the fomentation wrings itself. This is placed steaming hot over the affected area which has been first covered by a dry flannel. It is allowed to remain on for three or four minutes, and then another hot one wrung from the boiling water replaces the cool one. About four or five such applications are made. The skin should be very red at the close of this treatment. It is finished up with a quick, cold application to the reddened skin area.
The undressed child is placed upon a low stool in the half-filled bathtub at 100 F. with the feet in the warm water. A good lather is applied all over the body with good friction by the means of a shampoo brush and soap. He is then allowed to sit down in the tub and splash about all he pleases, rinse the soap off and allow him to have a good time generally. At the close of the treatment the water is cooled down and the treatment is finished with a brisk rub with the hands dipped in cold water. The skin of the child should be pink at the close of the treatment.
The moist abdominal bandage is indicated in such conditions as kidney inflammation which is so often seen in the second week of scarlet fever; or in congestion of any of the internal organs such as the liver, the stomach, intestines, etc., and is applied as follows: Spread out the flannel bandage and over it place the mackintosh. Wring dry the cotton strip from cold water, and spread it over the mackintosh. Wrap all three layers, the wet cloth next the skin, closely about the body, so as to prevent the air from getting under it. Be sure that the feet are warm while adjusting the bandage. In the morning remove the bandage, and rub the skin briskly with a turkish towel dipped in cold water, until the skin is pink and dry. The cotton strip should be boiled every other day to avoid skin eruptions.432
The heating compress is indicated in the following cases: Sprained ankles, rheumatic joints, arthritis, sore throat, etc. Directions: Wring two thicknesses of cheesecloth from cold water, place over the painful part, and quickly cover with a mackintosh and two thicknesses of woolen blanket bandage. On removing in the morning, sponge with cold water or alcohol.
In the bronchitis of small children, particularly babies, mustard pastes are to be preferred to the hot fomentations which are used to such great advantage in children above ten. The mustard paste is administered as follows: One part of mustard and six parts of flour of the same measurements are quickly stirred up with warm water to a paste thin enough to spread well upon a piece of thin muslin, which is large enough to cover twice the part to be treated. One-half of this muslin is thus covered with the mustard and the dry piece of cloth brought over. The edges are then folded in such a way that the mustard will not run out. This is applied to the affected part and allowed to remain for seven minutes on an infant, nine minutes on a child, and ten or twelve minutes on an adult. It is then removed and the moisture which is always seen on the reddened skin surface is not wiped off but talcum powder is sprinkled on thickly to absorb it. If this is done, a mustard paste may be repeated every two hours if necessary and no blistering or other harm will come to the skin.
The oil-silk jacket is used in bronchitis of babies and children. It consists of three layers, the innermost layer of cheesecloth, the middle layer of thin sheet wadding, and the outer layer of oil-silk. This jacket should comfortably cover the chest, front, and back; it has no sleeves, and is opened on the shoulder and under the arm. It should always follow the mustard paste in bronchitis. There should always be two433 such cheesecloth and cotton jackets with the oil-silk covering so they may be changed every twelve hours, thus allowing for airing.
1. Steam inhalations are indicated in hoarseness and bronchitis. They may be given in a number of ways. Perhaps that most convenient for the young infant is the "bronchitis tent." A sheet completely covers the crib, and, with the bed amply protected with rubber sheeting or an extra blanket, steam is allowed to enter under the sheet at the foot of the bed from a funnel put into the nose of the teakettle. The steam should continue for seven or eight minutes.
2. A large, heavy-paper funnel is put in the nose of the teakettle which is boiling on the gas range. The mother holds the child in her arms while she is enveloped with a sheet which also includes the funnel. A helper carefully guards the flame. The mother and baby may thus conveniently get the steam with very little difficulty.
3. For the older child or adult, steam inhalations are to be had from the ordinary croup kettle or from a twelve- or fourteen-inch tin can which is filled two-thirds full of boiling water. Over the top is loosely spread a cheesecloth upon which a few drops of compound tincture of benzoin or eucalyptus are sprinkled. The opened mouth is brought near the top of this can and a towel is thrown over the head, can and all; the patient thus being able satisfactorily to inhale the medicated steam.
Boric-Acid-and-Myrrh Lotion.
| Boric acid | 20 grains |
| Tincture of myrrh | ½ fluidrachm |
| Glycerine | 1 fluidrachm |
| Water, enough to make | 1 fluid ounce |
Apply frequently to the inside of the mouth for inflammation or thrush.
| Tannic acid | 2 drachms |
| Glycerine | 1 fluidrachm |
| Water | 2 fluid ounces |
To be injected or snuffed into the nose in obstinate cases of nosebleed.
Dobell's solution is an excellent throat gargle. A solution of half alcohol and half water is also a splendid gargle.
| Listerine | 2 teaspoons |
| Soda bicarbonate | 10 grains |
| Water | 4 ounces |
Essence of cinnamon, six drops in one-half glass cold water, may also be used in brushing the teeth and in cleansing the tongue and mouth.
1. Carbolic Acid.
| Carbolic acid (95%) | 6 ounces |
| Glycerine | 4 ounces |
| Water | 1 gallon |
Clothes should be soaked in this for several hours, then removed in a covered receptacle and boiled thoroughly. Sheets may be wet with this and hung at the doors in case of infectious diseases.
2. Chloride of Lime.
| Chloride of Lime | 4 ounces |
| Water (rain) | 1 gallon |
In typhoid fever, all the movements from the bowels should be thoroughly mixed with this, covered and allowed to stand several hours before pouring down the water closet. All vomited matter should be treated the same way.
There are a number of mush poultices recommended for different conditions—boils, felons, etc., but we find the aseptic435 heating compress to be as effectual as any of these dirty, mush poultices and we suggest that our readers try the boracic-acid poultice which is put on as follows: Over any infected area or abrasion of the skin a thick padding of cotton moistened by a saturated boracic-acid solution is placed. This is entirely covered with wax paper or oiled-silk, and held in place by a binder. It is sanitary and much to be preferred to any of the mush poultices of bygone days.
A very useful cough syrup may be made as follows: Two tablespoons of flaxseed are steeped on the stove until clear, the jelly strained and flavored quite sour with lemon juice to which is added rock candy for sweetening. This will often effectively relieve the irritating coughs of childhood.
| No. 1 | Glycerine | 3 ounces |
| Tr. Benzoin | ½ ouncs | |
| Water | 1 ounce |
| No. 2 | Glycerine | 2 ounces |
| Lemon juice | ½ ouncs | |
| Tr. Myrrh | ½ ounce |
| No. 3 | Glycerine | 2 ounces |
| Rose Water | 2 ouncs | |
| Acetic Acid | 2 ounce |
We wish to submit two very useful prescriptions for that troublesome skin disease which is so annoying in childhood as well as in adult life. Prescription No. 1 is a clear fluid, and after the affected area is thoroughly cleansed with resinol soap and rinsed in soft water, the lotion is applied and allowed to dry. No. 2 is then patted on with sterile cotton and often repeated to keep the eczematous skin area moist. This has proved curative in many persistent cases.436
Lotion No. 1.
| Acid Carbolic | 1 drachm |
| Listerine | 1 drachm |
| Rose Water | 3 ounces |
| Alcohol q. s. | 6 ounces |
Apply No. 1 and allow to dry of itself.
Lotion No. 2.
| Ichthyol | 4 drachms |
| Lime Water | 1 ounce |
| Oil sweet almonds | 1 ounce |
| Glycerine | 1½ ounces |
| Rose Water | 1½ ounces |
Apply No. 2 and repeat to keep moist.
CONSTIPATION
We submit the following home regime, which has proved successful to many sufferers for the treatment of constipation.
1. On rising in the morning, remove the moist abdominal bandage (mentioned above); drink two-thirds of a glass of cold water; and spend fifteen to twenty minutes in the following exercises, before dressing: Abdominal lifting with deep breathing, auto-massage, leg raising, trunk twisting, trunk bending—forward and to sides; lying down for the trunk raising, and sitting for the trunk circumduction. Immediately following these exercises, go to stool. Have feet raised from the floor eight or ten inches, in order to simulate the squatting position.
2. Breakfast should include bran or bran bread, and two or three of the following foods: Apples with skins, grapefruit, cranberries with skins (but little sugar), and figs. Immediately after breakfast walk fifteen minutes in the open air, practicing deep abdominal breathing. If the results at stool before breakfast were not satisfactory, vaseline rectum and go to stool again.
3. Lunch should consist of fruit only, while dinner should include bran bread and two of the following foods: Spinach, celery, carrots, parsnips, squash, or cabbage.437
4. Before retiring, walk in the open air for fifteen minutes; after undressing, exercise same as morning; and on retiring, apply the moist abdominal bandage.
| Poison. | Antidotes. | |
| Unknown | { | Emetic, followed by Jeaunel's antidote and soothing drinks. |
| Acid—acetic, hydrochloric, sulphuric, nitric |
{ | An alkali, such as magnesia, chalk, whiting, soda, soap; followed by soothing drinks or sweet oil. |
| Acid—carbolic, creosote | { | Epsom salts in abundance; soap; no oil. Dilute alcohol. |
| Acid—oxalic, including "salts of lemon" |
{ | Emetic, followed by lime (as chalk, plaster, whiting) or magnesia, but not by potash or soda; then soothing drinks. |
| Acid—prussic | { | Fresh air; ammonia to nostrils; cold douche; artificial respiration. |
| Aconite | { | Emetic, followed by digitalis; no pillow under head; free stimulation. |
| Alcohol (brandy, etc.) | { | Emetic; cold douche on head; warmth and artificial respiration. |
| Alkalies—ammonia, spirits of hartshorn, lye, caustic potash |
{ | Vinegar or lemon juice, followed by soothing drinks or sweet oil. |
| Antimony (tartar emetic). | { | Emetic if vomiting is not already profuse; then tannic acid freely, or strong tea; later, milk or other soothing drinks; finally, castor oil to empty the bowels.438 |
| Arsenic (Fowler's solution, Paris green, "Rough on Rats" |
{ | Emetic, quickly followed by plenty of a fresh mixture of the tincture of chloride of iron with calcined magnesia, washing or baking soda, or water of ammonia, or by Jeaunel's antidote. Then white of egg, soothing drinks, or sweet oil; castor oil to empty bowels. |
| Atropine (see Belladonna). | ||
| Belladonna (atropine) | { | Emetic; tannic acid freely; cold to head; coffee. Stimulants and warmth if needed. |
| Blue stone; blue vitriol (see Copper). |
||
| Chloral | { | Emetic (but often useless); external heat; stimulants; strong coffee; strychnine; atropine; artificial respiration. |
| Chloroform, inhaled | { | Cold douche; friction of skin; inverting child; artificial respiration. |
| Copper (blue stone; blue vitriol; verdigris) |
{ | Emetic, followed by white of egg or milk, yellow prussiate of potash; then soothing drinks. |
| Corrosive sublimate (bichlorid of mercury) |
{ | Emetic, followed by white of egg or milk; soothing drinks; tannic acid freely; castor oil to open bowels. |
| Cyanide of potash (see Acid, prussic). |
||
| Fowler's solution (see Arsenic). |
||
| Gas (illuminating gas, coal gas) |
{ | Inhalation of oxygen; artificial respiration; ammonia to nostrils; cold douche.439 |
| Iodine | { | Starch or flour mixed with water given freely; emetic; soothing drinks. |
| Laudanum (see Opium). | ||
| Lead (sugar of lead) | { | Emetic, followed by Epsom salts; white of egg or milk; alum. |
| Matches (see Phosphorus). | ||
| Morphine (see Opium). | ||
| Nux vomica (see Strychnine). | ||
| Opium (including laudanum, morphine, paregoric, soothing syrups, etc.) |
{ | Emetic (but generally useless); permanganate of potash in doses of 4 or 5 grains if case is seen early; strong coffee; atropine; keep child awake and breathing by cold douche to head and spine, walking, etc., but not to extent of exhaustion; artificial respiration. |
| Paregoric (see Opium). | ||
| Paris green (see Arsenic). | ||
| Phosphorus (match-heads, some roach and rat poisons) |
{ | Emetic; then permanganate of potash in doses of 4 or 5 grains well diluted, and frequently repeated; then Epsom salts or magnesia to open bowels, but no milk or oil of any kind. |
| Poisonous plants (Jimson weed, poisonous mushrooms, deadly nightshade, tobacco, etc.) |
{ | Emetic, followed by tannic acid; strong coffee or brandy; ammonia to nostrils; external warmth; artificial respiration.440 |
| Prussic acid (see Acid, prussic). |
||
| Silver nitrate (lunar caustic) | { | Table-salt, followed by emetic; milk or white of eggs. |
| Spoiled food | { | Emetic, followed by castor oil as purgative. |
| Strychnine (nux vomica, some rat poisons) |
{ | Emetic, followed by tannic acid, bromide of potash freely, or chloral. |
| Tartar emetic (see Antimony) | ||
At birth.
| Weight | 7½ pounds |
| Height | 20½ inches |
| Chest | 13½ inches |
| Head | 14 inches |
One year.
| Weight | 21 pounds |
| Height | 29 inches |
| Chest | 18 inches |
| Head | 18 inches |
Two years.
| Weight | 27 pounds |
| Height | 32 inches |
| Chest | 19 inches |
| Head | 19 inches |
Three years.
| Weight | 32 pounds |
| Height | 35 inches |
| Chest | 20 inches |
| Head | 19¼ inches |
Four years.
| Weight | 36 pounds |
| Height | 38 inches |
| Chest | 20¾ inches |
| Head | 19¾ inches |
Five years.
| Weight | 41 pounds |
| Height | 41½ inches |
| Chest | 21¾ inches |
| Head | 20¾ inches |
Six years.
| Weight | 45 pounds |
| Height | 44 inches |
| Chest | 23 inches |
Seven years.
| Weight | 49½ pounds |
| Height | 46 inches |
| Chest | 23½ inches |
Eight years.
| Weight | 54½ pounds |
| Height | 48 inches |
| Chest | 24½ inches |
Nine years.
| Weight | 60 pounds |
| Height | 50 inches |
| Chest | 25 inches |
Ten years.
| Weight | 66½ pounds |
| Height | 52 inches |
| Chest | 26 inches |
6 Weights for the first four years are without clothes, after that
with ordinary house clothes.
The weight of girls is on the average about one pound less than boys. They are about the same in height.
Ichthyol 5 per cent
Cocoa Butter q. s. ad. to make 24 suppositories.
Sig. Use one suppository in the rectum each evening for hemorrhoids.
The best way to administer an oil enema is by means of a special enema can which holds one pint, to which is attached a rubber tube. It is wise not to use an ordinary fountain syringe as the oil spoils the rubber very quickly. This oil is allowed to flow in slowly, under low pressure, and should be retained over night. Any oil is acceptable, the cheaper sweet oils will serve just as well as olive oil.442
| Diseases. | Incubation lasts— | Date of characteristic symptom from beginning of invasion. | Characteristic symptom. | Other principal symptoms. | Whole duration of disease from onset. | Quarantine lasts from onset. |
| Typhoid fever. | 7 to 10 days. | 7th or 8th day. | Rose-red, slightly elevated spots. | Apathy; diarrhœa; nosebleed; headache. | 2 to 4 weeks. | While disease lasts. |
| Scarlet fever. | 1 to 7 days. | 1st or 2d day. | Intense, bright-red blush over body. | Sore throat; often vomiting with onset. | 7 to 9 days or more (not including desquamation). | 6 weeks. |
| Measles. | 10 to 11 days. | 4th day. | Dusky or purplish-red, slightly elevated spots, scattered and in characteristic groupings. | Cold in head; running eyes; cough; hoarseness. | 7 to 8 days. | 3 weeks. |
| German measles. | 7 to 21 days. | 1st day. | Pale, rose-red spots or uniform blush; no characteristic groupings. | Slight sore throat; sometimes slight running of eyes and nose. | 3 to 4 days. | 3 weeks. |
| Chicken-pox. | 13 to 17 days. | 1st day. | Pea-sized, scattered vesicles. | None; or slight fever. | A week or less. | 3 to 4 weeks. |
| Varioloid (Variola). | 7 to 12 days. | 3d day (may be 1st or 2d). | Red, elevated papules; then vesicles; then often pustules. | Headache; backache; vomiting. | About 14 days. | 4 to 8 weeks. |
| Varioloid (Variola). | 7 to 12 days. | 3d day (may be 1st or 2d). | Red, elevated papules; then vesicles; then often pustules. | Headache; backache; vomiting. | About 14 days. | 4 to 8 weeks. |
| Vaccinia (Vaccination). | 1 to 3 days. | 1st day (3d after vaccination). | A red papule, becoming a vesicle and then a pustule; surrounded by a broad red area. | Often feverishness and malaise. | About 3 weeks. | None. |
| Erysipelas. | 3 to 7 days. | 1st or 2d day. | Bright-red blush; puffy skin; often vesicles. | Fever; pain. | 4 to 6 days, or several weeks if it spreads. | Averages 2 weeks. |
| Diphtheria. | 2 to 12 days. | 1st or 2d day. | White membrane on tonsils and other parts of throat. | Debility; fever. | 10 to 14 days. | 3 to 4 weeks. |
| Whooping-cough. | 2 to 7 days. | 7th to 14th day. | A prolonged paroxysm of coughing followed by a crowing inspiration (whoop). | Vomiting; spitting of blood. | 6 to 8 weeks. | 6 to 8 weeks (while whoop lasts). |
| Mumps. | 7 to 21 days. | 1st day. | Swelling in front, below, and behind the ear and below the jaw. | Pain when chewing. | A week or less. | 3 to 4 weeks. |
| Influenza. | Uncertain. Probably 1 to 7 days. | 1st day. | Fever, prostration. | Various respiratory, digestive, or nervous symptoms, commonest being general aching and cough. | 3 or 4 days to two weeks or more. | While disease lasts. |
The hot colonic flushing is particularly serviceable in combating the sick headaches of migraine. They should be taken at night just before retiring with the temperature of water as hot as can be borne, from 108 to 110 F. Half of the water is allowed to flow into the colon and is retained as long as possible. This brings the heat in close contact with the sympathetic nervous system whose headquarters is in the abdomen.
Position for an Enema. Lie on left side, knees brought up against abdomen, with the left arm well underneath. This will relax the abdominal muscles and allow the water to pass upward more freely. The water should be allowed to flow until it is felt low on the right side.
The one, two, three enema is an injection that is used for the relief of gas in the bowel. It consists of the following: One part epsom salts, two parts glycerine, and three parts soap suds. It is introduced by the aid of the colon tube and retained as long as is possible.
Glycerine and soapy water, equal parts, may be introduced into the bowel for temporary relief of a persistent constipation.
In instances when feeding by the mouth is impossible, nutrient enemas should be given every three or four hours during the day. The absorption does not take place in the large bowel as readily as in the small intestines, so only a small amount of a more highly concentrated solution is given at one time. A child one year of age will be given one teaspoon, from one to four years of age a teaspoon to a tablespoon is allowed, and up to twelve years from one to eight tablespoons are given in the nutrient enema. Peptonized meat preparations may be employed in greater concentration than directed by the use of the mouth. Peptonized milk containing an egg is often used. The pepsin is added to the mixture only when warm, and is injected at once.
1. A glass of warm water containing as much common table salt as can be dissolved.444
2. A teaspoon of mustard in a large glass of warm water.
3. A teaspoon of syrup of ipecac, repeated in fifteen minutes if necessary.
Any one of these emetics is useful in instances where it is desirable to empty the stomach at once.
A calorie is the heat unit used in the estimation of the fuel value of various foods. For instance, an ordinary slice of homemade bread contains 100 calories. An ordinary fig contains almost 100 calories. A large orange or an apple or a glass of grape juice contains about 100 calories. There are 100 calories in three teaspoons of sugar or honey.
A complete food list with the estimation of calorie value of foods is found in The Science of Living, page 370, while on page 99 of the same book is a very helpful table showing the amounts of various foods required to equal 100 calories. The reader will find this exceedingly practical in estimating food values for the household.
Since we find that in all acute diseases the acidity of the urine is greatly increased and in time of health it is less acid, we submit two lists of foods which tend to acidify the urine or to alkalinize the urine.
| FOODS WHICH TEND TO ACIDIFY |
FOODS WHICH TEND TO ALKALINIZE. |
|||
| 1. Animal Foods: All forms of flesh foods, fish, fowl, etc., including all kinds of meat broths, soups, beef tea, bouillon, etc. 2. Eggs. 3. Breadstuffs: All kinds of breads, whether made of wheat, rye or corn, crackers, toasts, griddle cakes, etc. 4. Pastries. All sorts of pies |
1. Dairy Products: Milk, ice cream, cottage cheese, cheese, buttermilk, etc. 2. Potatoes and bananas 3. Soups: All forms of vegetable and fruit soups and broths. 4. Fruit Juices: All the fresh fruit juices except plums. 5. Fresh Fruits: All fresh fruits, sweet and sour, except plums and cranberries.445 |
|||
| and cakes—except fruit pies, and other desserts containing milk or sour fruits. 5. Cereals: Rice, oatmeal, and breakfast foods of all kinds, including the flaked and toasted breakfast foods. 6. Peanuts, plums, prunes, and cranberries. Plums and cranberries fall in this column because of their benzoic acid, which the body cannot fully oxidize. |
6. Vegetables: All kinds, especially beets, carrots, celery, lettuce, and muskmelon. 7. Dried Fruits: Figs, raisins, dates, currants—all except prunes. 8. The Legumes: Beans, peas, and lentils. 9. The Nuts: All the nuts belong in this column, including almonds and chestnuts. |
It is often necessary to give the infant or the young child cereal water to replace food in occasions of summer diarrhoea, etc.
1. Barley Water.
One tablespoon of barley flour in one pint of water. Boil for
one-half hour, strain, and add sufficient boiled water to make
one pint.
2. Flaxseed Tea.
One tablespoon of flaxseed, one pint of boiling water; let
stand and keep warm for one hour; strain. Add juice of
lemon.
3. Oatmeal Jelly.
Four tablespoons of oatmeal, one pint of water; boil for
three hours in double boiler, adding water from time to time;
strain.
4. Toast Water.
One, two, or three slices of bread toasted dark brown, but
not burned. Put in one quart of boiling water, cover, and
strain when cold.
5. Arrowroot Water.
Wet two teaspoons of arrowroot with a little cold water, and
rub until smooth; then stir into one pint of boiling water and
boil for five minutes, stirring all the while.
6. Oatmeal Water.446
One tablespoon of oatmeal to one pint of boiling water, cover
and let simmer for one hour. Add water from time to time
as it evaporates; strain.
7. Rice Water.
One tablespoon of (washed) rice to one pint of water. Boil
three hours adding water from time to time.
Fruit juices are exceedingly beneficial all through life; particularly is this true during early childhood when the little ones are so likely to be constipated. Any of the fruit juices are good, particularly the juices from oranges, raisins, prunes, apples, pears, and cranberries. All these juices are better cooked than raw with the exception of orange juice. All children should have some fruit juice every day. For the very young baby the juices are strained through a wire strainer and a clean cheesecloth so as to remove every particle of solid matter, and there should be added an equal amount of cold, boiled water for the infant under ten months.
Lemonade, along with orangeade, grapefruitade and limeade should be used for children above a year. They should be well diluted and not too sweet.
Eggnogs are splendid for children who need to be helped along with their diet. They may be given at the close of the meal, never between meals—unless so prescribed by a physician. The stomach should have ample time to complete the work of digesting one meal before another partial meal is allowed to enter it. Eggnogs consist of a well-beaten egg into which there is placed a small amount of sugar, flavoring with either nutmeg, vanilla, or cinnamon, and the glass filled up with rich milk.
Milkshake is a delightful drink. The white of an egg with one or two teaspoons of sugar, two tablespoons of chopped ice,447 flavoring, and one ounce of cream are briskly shaken in a milk-shaker for two minutes. Cold milk is added to fill the glass.
Beef extracts are regarded by the medical profession as purely stimulants. Beef juice is practically without food value. In the preparation of beef juice the extractives and juices leave the fibre. The food is in the fibre of the meat. The extractives are purely of a stimulating order. We do not advocate the giving of beef tea and beef juices to children; as a rule, we think that cereal, gruels, strained soups, and milk are preferable.
The only reason for cooking meats is to destroy the parasites such as tapeworm, trichina, etc., which are so often found in the meat. The cooking of meat decreases its digestibility, as raw meat is more easily digested than cooked meat, but we feel it is necessary to advocate the cooking of meat in order to kill the parasites.
A fresh egg, shell on, is placed in boiling water which is immediately after removed from the fire. The egg then cooks slowly in the water, which gradually cools, for seven or eight minutes, when the white should be about the consistency of jelly. For a delicate digestion the white only should be given, with salt; it can be easily separated from the yolk. The above is the best form of egg for the young child. Later on the eggs may be soft boiled or poached, or even soft scrambled.
Two varieties of soups are given children. In the early months of childhood, from six years to eighteen months, the soups are usually strained, but after eighteen months, soups may be thickened with flour and rich milk making a cream soup of it. Most vegetables make good soups. The pulp from such vegetables as asparagus, carrots, beans, peas, tomatoes, and potatoes are made into cream soups by the addition of a little flour, rich milk, butter, and a dash of salt.448
New breads should never be given to a child. Only bread twenty-four hours old should ever be given to a child under six years; it should be cut into slices and allowed to dry out; and even then is better if slightly toasted. We publish a recipe for bran bread and bran biscuits which are exceedingly good for children and adults.
Recipe for Bran Bread. Two eggs, beaten separately; three-fourths of a cup of molasses, with one round teaspoon soda; one cup of sour cream; one cup of sultana seedless raisins; one cup of wheat flour, with one heaping teaspoon baking powder; two cups of bran; stir well and bake one hour.
Bran Biscuits. Mix one pint of bran, one-half pint of flour, and one level teaspoon of baking soda. Mix one-half pint of milk and four tablespoons of molasses. Add this to the bran mixture and bake in gem pans.
| A | B | C | D | E | F | G | H | I | J | K | L | M |
| N | O | P | Q | R | S | T | U | V | W | X | Y | Z |
End of the Project Gutenberg EBook of The Mother and Her Child, by
William S. Sadler and Lena K. Sadler
*** END OF THIS PROJECT GUTENBERG EBOOK THE MOTHER AND HER CHILD ***
***** This file should be named 20817-h.htm or 20817-h.zip *****
This and all associated files of various formats will be found in:
http://www.gutenberg.org/2/0/8/1/20817/
Produced by Audrey Longhurst, Hillie Plantinga and the
Online Distributed Proofreading Team at http://www.pgdp.net
Updated editions will replace the previous one--the old editions
will be renamed.
Creating the works from public domain print editions means that no
one owns a United States copyright in these works, so the Foundation
(and you!) can copy and distribute it in the United States without
permission and without paying copyright royalties. Special rules,
set forth in the General Terms of Use part of this license, apply to
copying and distributing Project Gutenberg-tm electronic works to
protect the PROJECT GUTENBERG-tm concept and trademark. Project
Gutenberg is a registered trademark, and may not be used if you
charge for the eBooks, unless you receive specific permission. If you
do not charge anything for copies of this eBook, complying with the
rules is very easy. You may use this eBook for nearly any purpose
such as creation of derivative works, reports, performances and
research. They may be modified and printed and given away--you may do
practically ANYTHING with public domain eBooks. Redistribution is
subject to the trademark license, especially commercial
redistribution.
*** START: FULL LICENSE ***
THE FULL PROJECT GUTENBERG LICENSE
PLEASE READ THIS BEFORE YOU DISTRIBUTE OR USE THIS WORK
To protect the Project Gutenberg-tm mission of promoting the free
distribution of electronic works, by using or distributing this work
(or any other work associated in any way with the phrase "Project
Gutenberg"), you agree to comply with all the terms of the Full Project
Gutenberg-tm License (available with this file or online at
http://gutenberg.org/license).
Section 1. General Terms of Use and Redistributing Project Gutenberg-tm
electronic works
1.A. By reading or using any part of this Project Gutenberg-tm
electronic work, you indicate that you have read, understand, agree to
and accept all the terms of this license and intellectual property
(trademark/copyright) agreement. If you do not agree to abide by all
the terms of this agreement, you must cease using and return or destroy
all copies of Project Gutenberg-tm electronic works in your possession.
If you paid a fee for obtaining a copy of or access to a Project
Gutenberg-tm electronic work and you do not agree to be bound by the
terms of this agreement, you may obtain a refund from the person or
entity to whom you paid the fee as set forth in paragraph 1.E.8.
1.B. "Project Gutenberg" is a registered trademark. It may only be
used on or associated in any way with an electronic work by people who
agree to be bound by the terms of this agreement. There are a few
things that you can do with most Project Gutenberg-tm electronic works
even without complying with the full terms of this agreement. See
paragraph 1.C below. There are a lot of things you can do with Project
Gutenberg-tm electronic works if you follow the terms of this agreement
and help preserve free future access to Project Gutenberg-tm electronic
works. See paragraph 1.E below.
1.C. The Project Gutenberg Literary Archive Foundation ("the Foundation"
or PGLAF), owns a compilation copyright in the collection of Project
Gutenberg-tm electronic works. Nearly all the individual works in the
collection are in the public domain in the United States. If an
individual work is in the public domain in the United States and you are
located in the United States, we do not claim a right to prevent you from
copying, distributing, performing, displaying or creating derivative
works based on the work as long as all references to Project Gutenberg
are removed. Of course, we hope that you will support the Project
Gutenberg-tm mission of promoting free access to electronic works by
freely sharing Project Gutenberg-tm works in compliance with the terms of
this agreement for keeping the Project Gutenberg-tm name associated with
the work. You can easily comply with the terms of this agreement by
keeping this work in the same format with its attached full Project
Gutenberg-tm License when you share it without charge with others.
1.D. The copyright laws of the place where you are located also govern
what you can do with this work. Copyright laws in most countries are in
a constant state of change. If you are outside the United States, check
the laws of your country in addition to the terms of this agreement
before downloading, copying, displaying, performing, distributing or
creating derivative works based on this work or any other Project
Gutenberg-tm work. The Foundation makes no representations concerning
the copyright status of any work in any country outside the United
States.
1.E. Unless you have removed all references to Project Gutenberg:
1.E.1. The following sentence, with active links to, or other immediate
access to, the full Project Gutenberg-tm License must appear prominently
whenever any copy of a Project Gutenberg-tm work (any work on which the
phrase "Project Gutenberg" appears, or with which the phrase "Project
Gutenberg" is associated) is accessed, displayed, performed, viewed,
copied or distributed:
This eBook is for the use of anyone anywhere at no cost and with
almost no restrictions whatsoever. You may copy it, give it away or
re-use it under the terms of the Project Gutenberg License included
with this eBook or online at www.gutenberg.org
1.E.2. If an individual Project Gutenberg-tm electronic work is derived
from the public domain (does not contain a notice indicating that it is
posted with permission of the copyright holder), the work can be copied
and distributed to anyone in the United States without paying any fees
or charges. If you are redistributing or providing access to a work
with the phrase "Project Gutenberg" associated with or appearing on the
work, you must comply either with the requirements of paragraphs 1.E.1
through 1.E.7 or obtain permission for the use of the work and the
Project Gutenberg-tm trademark as set forth in paragraphs 1.E.8 or
1.E.9.
1.E.3. If an individual Project Gutenberg-tm electronic work is posted
with the permission of the copyright holder, your use and distribution
must comply with both paragraphs 1.E.1 through 1.E.7 and any additional
terms imposed by the copyright holder. Additional terms will be linked
to the Project Gutenberg-tm License for all works posted with the
permission of the copyright holder found at the beginning of this work.
1.E.4. Do not unlink or detach or remove the full Project Gutenberg-tm
License terms from this work, or any files containing a part of this
work or any other work associated with Project Gutenberg-tm.
1.E.5. Do not copy, display, perform, distribute or redistribute this
electronic work, or any part of this electronic work, without
prominently displaying the sentence set forth in paragraph 1.E.1 with
active links or immediate access to the full terms of the Project
Gutenberg-tm License.
1.E.6. You may convert to and distribute this work in any binary,
compressed, marked up, nonproprietary or proprietary form, including any
word processing or hypertext form. However, if you provide access to or
distribute copies of a Project Gutenberg-tm work in a format other than
"Plain Vanilla ASCII" or other format used in the official version
posted on the official Project Gutenberg-tm web site (www.gutenberg.org),
you must, at no additional cost, fee or expense to the user, provide a
copy, a means of exporting a copy, or a means of obtaining a copy upon
request, of the work in its original "Plain Vanilla ASCII" or other
form. Any alternate format must include the full Project Gutenberg-tm
License as specified in paragraph 1.E.1.
1.E.7. Do not charge a fee for access to, viewing, displaying,
performing, copying or distributing any Project Gutenberg-tm works
unless you comply with paragraph 1.E.8 or 1.E.9.
1.E.8. You may charge a reasonable fee for copies of or providing
access to or distributing Project Gutenberg-tm electronic works provided
that
- You pay a royalty fee of 20% of the gross profits you derive from
the use of Project Gutenberg-tm works calculated using the method
you already use to calculate your applicable taxes. The fee is
owed to the owner of the Project Gutenberg-tm trademark, but he
has agreed to donate royalties under this paragraph to the
Project Gutenberg Literary Archive Foundation. Royalty payments
must be paid within 60 days following each date on which you
prepare (or are legally required to prepare) your periodic tax
returns. Royalty payments should be clearly marked as such and
sent to the Project Gutenberg Literary Archive Foundation at the
address specified in Section 4, "Information about donations to
the Project Gutenberg Literary Archive Foundation."
- You provide a full refund of any money paid by a user who notifies
you in writing (or by e-mail) within 30 days of receipt that s/he
does not agree to the terms of the full Project Gutenberg-tm
License. You must require such a user to return or
destroy all copies of the works possessed in a physical medium
and discontinue all use of and all access to other copies of
Project Gutenberg-tm works.
- You provide, in accordance with paragraph 1.F.3, a full refund of any
money paid for a work or a replacement copy, if a defect in the
electronic work is discovered and reported to you within 90 days
of receipt of the work.
- You comply with all other terms of this agreement for free
distribution of Project Gutenberg-tm works.
1.E.9. If you wish to charge a fee or distribute a Project Gutenberg-tm
electronic work or group of works on different terms than are set
forth in this agreement, you must obtain permission in writing from
both the Project Gutenberg Literary Archive Foundation and Michael
Hart, the owner of the Project Gutenberg-tm trademark. Contact the
Foundation as set forth in Section 3 below.
1.F.
1.F.1. Project Gutenberg volunteers and employees expend considerable
effort to identify, do copyright research on, transcribe and proofread
public domain works in creating the Project Gutenberg-tm
collection. Despite these efforts, Project Gutenberg-tm electronic
works, and the medium on which they may be stored, may contain
"Defects," such as, but not limited to, incomplete, inaccurate or
corrupt data, transcription errors, a copyright or other intellectual
property infringement, a defective or damaged disk or other medium, a
computer virus, or computer codes that damage or cannot be read by
your equipment.
1.F.2. LIMITED WARRANTY, DISCLAIMER OF DAMAGES - Except for the "Right
of Replacement or Refund" described in paragraph 1.F.3, the Project
Gutenberg Literary Archive Foundation, the owner of the Project
Gutenberg-tm trademark, and any other party distributing a Project
Gutenberg-tm electronic work under this agreement, disclaim all
liability to you for damages, costs and expenses, including legal
fees. YOU AGREE THAT YOU HAVE NO REMEDIES FOR NEGLIGENCE, STRICT
LIABILITY, BREACH OF WARRANTY OR BREACH OF CONTRACT EXCEPT THOSE
PROVIDED IN PARAGRAPH F3. YOU AGREE THAT THE FOUNDATION, THE
TRADEMARK OWNER, AND ANY DISTRIBUTOR UNDER THIS AGREEMENT WILL NOT BE
LIABLE TO YOU FOR ACTUAL, DIRECT, INDIRECT, CONSEQUENTIAL, PUNITIVE OR
INCIDENTAL DAMAGES EVEN IF YOU GIVE NOTICE OF THE POSSIBILITY OF SUCH
DAMAGE.
1.F.3. LIMITED RIGHT OF REPLACEMENT OR REFUND - If you discover a
defect in this electronic work within 90 days of receiving it, you can
receive a refund of the money (if any) you paid for it by sending a
written explanation to the person you received the work from. If you
received the work on a physical medium, you must return the medium with
your written explanation. The person or entity that provided you with
the defective work may elect to provide a replacement copy in lieu of a
refund. If you received the work electronically, the person or entity
providing it to you may choose to give you a second opportunity to
receive the work electronically in lieu of a refund. If the second copy
is also defective, you may demand a refund in writing without further
opportunities to fix the problem.
1.F.4. Except for the limited right of replacement or refund set forth
in paragraph 1.F.3, this work is provided to you 'AS-IS' WITH NO OTHER
WARRANTIES OF ANY KIND, EXPRESS OR IMPLIED, INCLUDING BUT NOT LIMITED TO
WARRANTIES OF MERCHANTIBILITY OR FITNESS FOR ANY PURPOSE.
1.F.5. Some states do not allow disclaimers of certain implied
warranties or the exclusion or limitation of certain types of damages.
If any disclaimer or limitation set forth in this agreement violates the
law of the state applicable to this agreement, the agreement shall be
interpreted to make the maximum disclaimer or limitation permitted by
the applicable state law. The invalidity or unenforceability of any
provision of this agreement shall not void the remaining provisions.
1.F.6. INDEMNITY - You agree to indemnify and hold the Foundation, the
trademark owner, any agent or employee of the Foundation, anyone
providing copies of Project Gutenberg-tm electronic works in accordance
with this agreement, and any volunteers associated with the production,
promotion and distribution of Project Gutenberg-tm electronic works,
harmless from all liability, costs and expenses, including legal fees,
that arise directly or indirectly from any of the following which you do
or cause to occur: (a) distribution of this or any Project Gutenberg-tm
work, (b) alteration, modification, or additions or deletions to any
Project Gutenberg-tm work, and (c) any Defect you cause.
Section 2. Information about the Mission of Project Gutenberg-tm
Project Gutenberg-tm is synonymous with the free distribution of
electronic works in formats readable by the widest variety of computers
including obsolete, old, middle-aged and new computers. It exists
because of the efforts of hundreds of volunteers and donations from
people in all walks of life.
Volunteers and financial support to provide volunteers with the
assistance they need, is critical to reaching Project Gutenberg-tm's
goals and ensuring that the Project Gutenberg-tm collection will
remain freely available for generations to come. In 2001, the Project
Gutenberg Literary Archive Foundation was created to provide a secure
and permanent future for Project Gutenberg-tm and future generations.
To learn more about the Project Gutenberg Literary Archive Foundation
and how your efforts and donations can help, see Sections 3 and 4
and the Foundation web page at http://www.pglaf.org.
Section 3. Information about the Project Gutenberg Literary Archive
Foundation
The Project Gutenberg Literary Archive Foundation is a non profit
501(c)(3) educational corporation organized under the laws of the
state of Mississippi and granted tax exempt status by the Internal
Revenue Service. The Foundation's EIN or federal tax identification
number is 64-6221541. Its 501(c)(3) letter is posted at
http://pglaf.org/fundraising. Contributions to the Project Gutenberg
Literary Archive Foundation are tax deductible to the full extent
permitted by U.S. federal laws and your state's laws.
The Foundation's principal office is located at 4557 Melan Dr. S.
Fairbanks, AK, 99712., but its volunteers and employees are scattered
throughout numerous locations. Its business office is located at
809 North 1500 West, Salt Lake City, UT 84116, (801) 596-1887, email
business@pglaf.org. Email contact links and up to date contact
information can be found at the Foundation's web site and official
page at http://pglaf.org
For additional contact information:
Dr. Gregory B. Newby
Chief Executive and Director
gbnewby@pglaf.org
Section 4. Information about Donations to the Project Gutenberg
Literary Archive Foundation
Project Gutenberg-tm depends upon and cannot survive without wide
spread public support and donations to carry out its mission of
increasing the number of public domain and licensed works that can be
freely distributed in machine readable form accessible by the widest
array of equipment including outdated equipment. Many small donations
($1 to $5,000) are particularly important to maintaining tax exempt
status with the IRS.
The Foundation is committed to complying with the laws regulating
charities and charitable donations in all 50 states of the United
States. Compliance requirements are not uniform and it takes a
considerable effort, much paperwork and many fees to meet and keep up
with these requirements. We do not solicit donations in locations
where we have not received written confirmation of compliance. To
SEND DONATIONS or determine the status of compliance for any
particular state visit http://pglaf.org
While we cannot and do not solicit contributions from states where we
have not met the solicitation requirements, we know of no prohibition
against accepting unsolicited donations from donors in such states who
approach us with offers to donate.
International donations are gratefully accepted, but we cannot make
any statements concerning tax treatment of donations received from
outside the United States. U.S. laws alone swamp our small staff.
Please check the Project Gutenberg Web pages for current donation
methods and addresses. Donations are accepted in a number of other
ways including checks, online payments and credit card donations.
To donate, please visit: http://pglaf.org/donate
Section 5. General Information About Project Gutenberg-tm electronic
works.
Professor Michael S. Hart is the originator of the Project Gutenberg-tm
concept of a library of electronic works that could be freely shared
with anyone. For thirty years, he produced and distributed Project
Gutenberg-tm eBooks with only a loose network of volunteer support.
Project Gutenberg-tm eBooks are often created from several printed
editions, all of which are confirmed as Public Domain in the U.S.
unless a copyright notice is included. Thus, we do not necessarily
keep eBooks in compliance with any particular paper edition.
Most people start at our Web site which has the main PG search facility:
http://www.gutenberg.org
This Web site includes information about Project Gutenberg-tm,
including how to make donations to the Project Gutenberg Literary
Archive Foundation, how to help produce our new eBooks, and how to
subscribe to our email newsletter to hear about new eBooks.